Fig. 27.1
(a) Left atriotomy: using robotic curved scissors and Rosano forceps, the inter-atrial groove grove must be developed medial to right pulmonary veins. One has to be certain that the right pulmonary veins are lateral to this incision and that the incision is made within the body of the left atrium. The oblique sinus should be opened as to delineate the margin of the right atrium. (b) Cryoprobe deployment: using two EndoWrist™ robotic cardiac probe graspers the console surgeon can mold the malleable probe (3-mm OD) to customize cryolesions. Moreover, these instruments are used to compress the probe against atrial tissue
Left Atrial Cryo-Lesions
To provide dynamic access to the pulmonary veins (PV) and mitral valve, the robotic Endowrist™ dynamic left atrial retractor is positioned and directed along the inter-atrial septum with ventral displacement. After all four pulmonary veins, the mitral valve, and the left atrial appendage are visualized, 2 min endocardial freeze lesions are made in the following sequence:. The first lesion begins at the inferior aspect of the left atriotomy and extends around the left inferior PV (Fig. 27.2a). Generally, this lesion extends from lower side of the atriotomy around both right lower and most of the left lower PV.
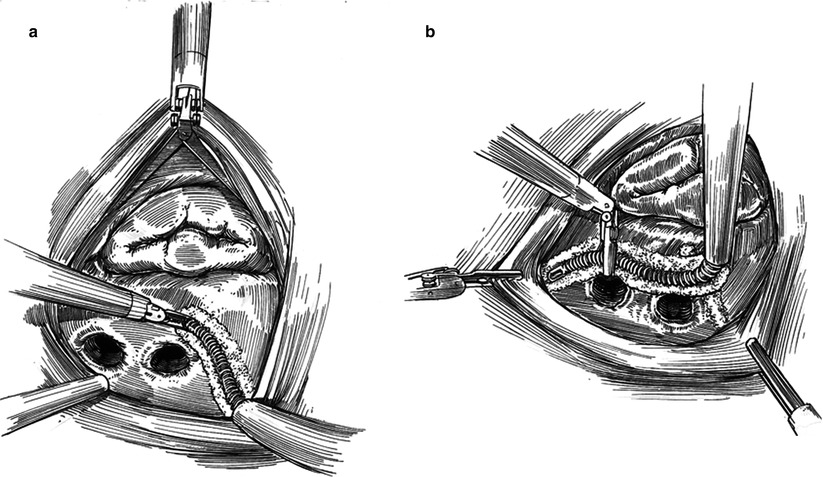
Fig. 27.2
Left atrial ablation. (a) The left atriotomy partially isolates the right pulmonary veins. To extend the ablation, the first cryolesion is placed from the lower edge of the atriotomy extending counterclockwise around both the right inferior pulmonary vein and part of the left inferior vein. (b) The second lesion extends counterclockwise from the prior lesion overlapping it. This lesion usually will isolate the left upper pulmonary vein. Generally, adequate freezing occurs between this vein and the base of the atrial appendage
The second lesion overlaps that of the left inferior PV and passes counterclockwise around the left superior PV, passing just inferior to the base of left atrial appendage (Fig. 27.2b). Generally, tissue between the left atrial appendage and the left superior PV is also frozen, obviating the need for a separate peri-appendage lesion. The third lesion is made in a clockwise direction and connects the last lesion (left superior PV) to the superior left atriotomy edge, completing the pulmonary vein “box lesion set” (Fig. 27.3a).
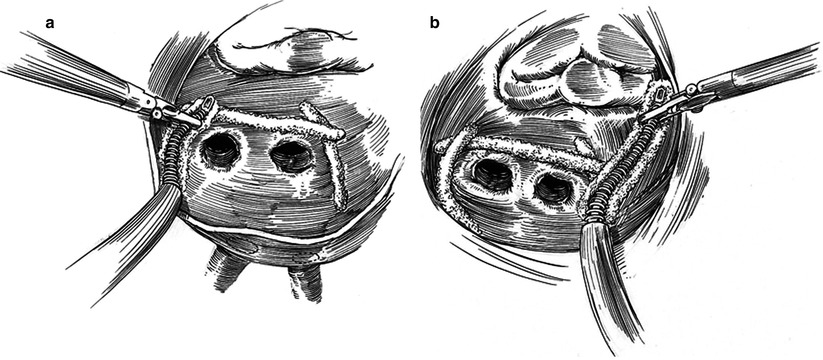
Fig. 27.3
Left atrial ablation. (a) The third lesion completes the “box lesion” around the pulmonary veins. The probe extends clockwise from the upper aspect of the atriotomy and around the left upper pulmonary vein, overlaps the second lesion. Usually, three contiguous cryolesions are require for a well made “box lesion”. (b) Beginning at the mid-portion of the first, the fourth lesion crossed the left atrial isthmus to the mitral valve annulus at P3. Often part of P3 becomes frozen indicating a complete lesion
The mitral isthmus lesion connects the pulmonary vein “box lesion” to the valve annulus, near the posterior leaflet P3 scallop (Fig. 27.3b). This fourth lesion must include the mitral P3 scallop base as incomplete lesions here often result in troublesome left atrial flutter. This lesion should be aimed towards P3 and not P2 in order to minimize the potential for injuring the circumflex coronary artery. To date, we have not had a permanent coronary artery or leaflet injury using this cryo-technique.
Using the oblique sinus for posterior left atrial access, the fifth lesion is applied across the coronary sinus (Fig. 27.4). Occasionally, the coronary sinus cannot be visualized because of covering fat. In this instance the atrio-ventricular groove must be crossed to be sure that the coronary sinus has been included. Retrograde coronary sinus cardioplegia catheters should be removed before freezing.

Fig. 27.4




Left atrial ablation. To make the fifth lesion across the coronary sinus, the cryoprobe is passed behind the inferior vena cava and through the oblique sinus. If the coronary sinus is obscured by fat, the probe should be passed well beyond the atrio-ventricular groove. Any retrograde coronary sinus cardioplegia catheter should be removed before freezing
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
