Chapter 61
Traumatic Heart Disease
1. What is the most common cause of cardiac injury?
Motor vehicle accidents are the most common cause of cardiac injury.
2. List the physical mechanisms of injury in cardiac trauma.
3. What is myocardial contusion?
4. Which major cardiovascular structures are most commonly involved in cardiac trauma?
Cardiac trauma most commonly involves traumatic contusion or rupture of the right ventricle (RV), aortic valve tear, left ventricle (LV) or left atrial rupture, innominate artery avulsion, aortic isthmus rupture (Fig. 61-1), left subclavian artery traumatic occlusion, and tricuspid valve tear.
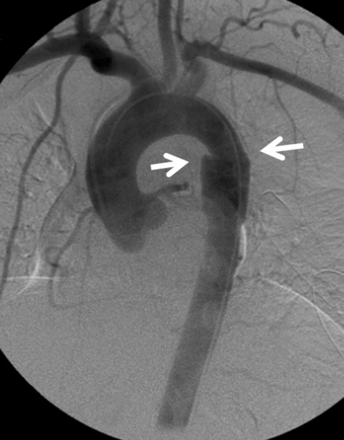
Figure 61-1 Traumatic rupture of the descending thoracic aorta (arrows) at the aortic isthmus. Modified from Valji K: Vascular and Interventional Radiology, ed 2, Philadelphia, 2006, Saunders.
5. What bedside findings can be detected in patients with suspected major cardiovascular trauma?
Obvious clinical signs in patients with nonpenetrating trauma are rare. However, a bedside evaluation by an astute clinician to detect possible life-threatening cardiovascular and thoracic complications can reveal important signs in just a few minutes (Table 61-1).
TABLE 61-1
IMPORTANT SIGNS OF CARDIOVASCULAR AND THORACIC TRAUMA
| Finding | Suggested Lesions |
| Pale skin color, conjunctiva, palms, and oral mucosa | Suggests important blood loss |
| Decreased blood pressure in the left arm | Seen in patients with traumatic rupture of the aortic isthmus, pseudocoarctation, or traumatic thrombosis of the left subclavian artery |
| Decreased blood pressure in the right arm | Consider innominate artery avulsion |
| Subcutaneous emphysema and tracheal deviation | Consider pneumothorax |
| Elevated jugular venous pulse with inspiratory raise (i.e., the Kussmaul sign) | Suggests cardiac tamponade or tension pneumothorax |
| Prominent systolic V wave in the venous pulse examination | Suggests tricuspid insufficiency as a result of tricuspid valve tear |
| Nonpalpable apex or distant heart sounds | Suspect cardiac tamponade |
| Pericardial rub | Diagnostic for pericarditis |
| Pulsus paradoxus | Seen in patients with cardiac tamponade, massive pulmonary embolism, or tension pneumothorax |
| Continuous murmurs or thrills | Consider traumatic arteriovenous fistula or rupture of the sinus of Valsalva |
| Harsh holosystolic murmurs | Suspect traumatic ventricular septal defect |
| Early diastolic murmur and widened pulse pressure | Suspect aortic valve injury |
| Cervical and supraclavicular hematomas | Seen in traumatic carotid rupture |
| New focal neurological symptoms | Traumatic carotid, aortic, or great vessel dissection |
6. Can an acute myocardial infarction complicate cardiac trauma?
7. What is the most common type of myocardial infarction suffered in trauma victims?
According to the universal definition of myocardial infarction, patients who have myocardial necrosis during trauma usually suffer a type 2 myocardial infarction. This type of myocardial necrosis is secondary to direct trauma or ischemia, and is a result of a relative imbalance of either increased myocardial oxygen demand or decreased myocardial oxygen supply (e.g., coronary artery spasm, coronary embolism, anemia, arrhythmias, hypertension, anemia, or hypotension), rather than coronary occlusion caused by advanced atherosclerosis or an acute coronary thrombotic event (type 1 myocardial infarction), and is characterized by a variable increase in cardiac biomarkers with no ischemic symptoms or ECG changes.
8. What is the preferred treatment for an ST elevation acute myocardial infarction in the event of chest trauma?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


