Transesophageal Sequential Analysis of Cardiovascular Segments in Diagnosis of Complex Congenital Heart Disease
Jesus Vargas-Barron
Clara Andrea Vazquez-Antona
Angel Romero-Cardenas
Francisco-Javier Roldan
Julio Erdmenger Orellana
Navin C. Nanda
Echocardiographic diagnosis of complex congenital heart disease requires a systematized study that is most logical if based on the sequential identification of the principal cardiovascular segments. It is advisable to begin the echocardiographic exploration with an evaluation of the atrial segments, followed by the ventricles and, finally, the great vessels. With the information obtained it is possible to define the types of intersegmental connections, that is, atrioventricular (A–V) and ventriculoarterial (V–A) connections.
When the atrial segment is examined, situs should be determined. Atrial situs indicates the morphology of the atria. When the atria have different morphologies, situs is solitus or inversus. The situation in which both atria have the same morphology is known as right or left atrial isomerism.
There are various methods of recognizing atrial situs, such as electrocardiography and, particularly, through bronchial morphology as observed in radiologic studies. Examination of other viscera, specifically the main lobe of the liver, is of no value, because in about half of the patients with complex congenital heart disease there is a discrepancy between atrial situs and visceral situs.
At present, the identification of atrial situs is considered reliable if it is based on a morphologic examination of the atrial appendages. Transesophageal echocardiography has facilitated the noninvasive diagnosis of atrial situs by permitting visualization of the appendages and of systemic and pulmonary venous return or other anatomic signs originating from embryonic remains.
There are four possible variants of atrial situs: (a) situs solitus, in which the morphologically right atrium is found on the right and the morphologically left atrium on the left; (b) situs inversus, in which the right atrium is located on the left and the left atrium on the right; and (c) right atrial isomerism or (d) left atrial isomerism, also known as situs ambiguous, in which both atria have a right or left morphology.
Once the atrial situs is determined, the ventricles must be identified to establish the A–V connection. Two well-developed ventricles can exist, or there may be one main ventricle and a rudimentary one, or, less frequently, a true single ventricle. When there are two well-developed ventricles, the tricuspid valve always accompanies the morphologically right ventricle and the mitral valve accompanies the morphologically left ventricle.
After the atrial and ventricular segments have been identified, the type of A–V connection can be established. The possible variations include the following: (a) concordant A–V connection, in which the right atrium is connected to the right ventricle and the left atrium to the left ventricle, regardless of their spatial relationships; (b) discordant A–V connection, in which the right atrium is connected to the left ventricle and vice versa; (c) ambiguous A–V connection, in which in the presence of right or left isomerism, the separate atrial cavities or a common atrial chamber connect with the two ventricles; (d) double ventricular inlet, in which the two atria are connected to the same ventricular cavity; and (e) absence of right or left A–V connection, in which a single A–V valve connects an atrium with the main ventricular cavity and the other atrium has no ventricular connection.
In addition to identifying the type of A–V connection, echocardiographic exploration helps define the mode of this connection. The connection between atria and ventricles can be made (a) by means of two perforate valves, (b) by one perforate valve and one imperforate valve, or (c) by an overriding and straddling A–V valve.
The next step is to identify the great vessels and establish the type of V–A connection. The identification of the great vessels can be achieved by examining their anatomy and trajectory as they emerge from the heart using two-dimensional imaging. The aorta continues cephalad, parallel to the sternum, until it reaches the aortic arch, from which the supra-aortic vessels originate. In contrast, the pulmonary artery has a short course, because it takes a posterior direction and rapidly bifurcates. The possible variations are as follows: (a) concordant V–A connection, in which the left ventricle is connected to the aorta and the right ventricle to the pulmonary artery; (b) discordant V–A connection, in which the left ventricle is connected to the pulmonary artery and the right ventricle to the aorta; (c) double ventricular outlet, in which both semilunar orifices are connected in >50% of their diameter with one ventricle, usually the morphologically right ventricle; and (d) univentricular outlet, in which a single artery emerges from the heart, as in the case of truncus arteriosus or pulmonary or aortic atresia.
Once the echocardiographic diagnosis of V–A connection has been established, the mode of connection—which can be with two perforate valves, with one perforate valve and one imperforate valve, with overriding valves, or with a common valve—should also be clarified.
The rest of this chapter discusses the use of transesophageal echocardiography in the study of congenital malformations of the heart, using sequential segmental diagnosis in the description.
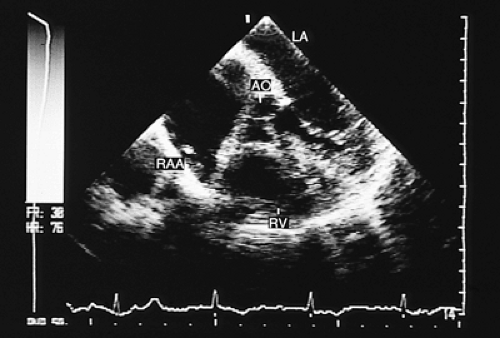 FIGURE 8.2.1. Situs solitus. Transverse plane image demonstrates the normal morphology of the right atrial appendage (RAA). AO, aorta; LA, left atrium; RV, right ventricle. |
Atrial Situs
Situs Solitus
Transesophageal studies in transverse and longitudinal planes allow the identification of the cardiac structures and chambers.
The right atrial appendage has a triangular morphology with a large implantation base connecting it to the atrial cavity (1). (Fig. 8.2.1). In transverse plane images the crista terminalis of the right atrium can be seen as a prominence separating the appendage, with its pectineal musculature, from the smooth atrial portion (Fig. 8.2.1). The right atrium receives the systemic venous return, and the connection with the superior vena cava can be observed in progressive sections in the transverse plane (Fig. 8.2.2). It is possible to see the connections of both venae cavae with images in the longitudinal plane. Transgastric recordings show the connection of the suprahepatic veins to the inferior vena cava and its communication with the right atrium.
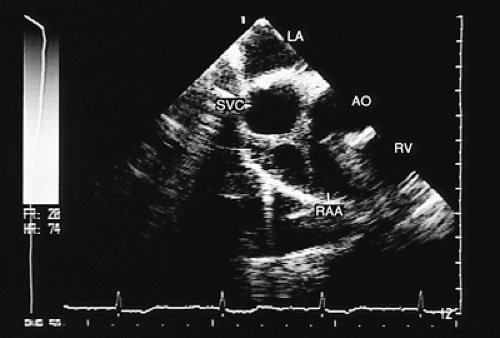 FIGURE 8.2.2. Situs solitus. In this transverse plane image the connection of the superior vena cava (SVC) to the right atrium can be observed. AO, aorta; LA, left atrium; RAA, right atrial appendage; RV, right ventricle. |
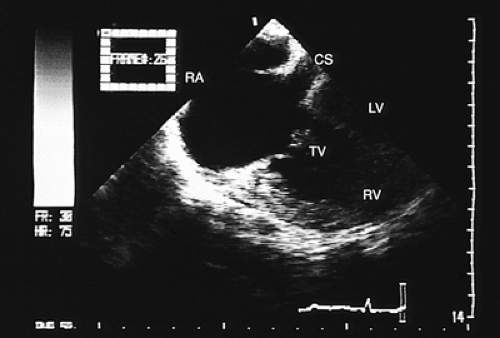 FIGURE 8.2.3. Situs solitus. Transverse plane image of the four chambers with posterior angulation demonstrates the normal drainage of the coronary sinus (CS) into the right atrium (RA). LV, left ventricle; RV, right ventricle; TV, tricuspid valve. |
Starting with a four-chamber image, posterior angulation of the probe allows visualization of the coronary sinus, which crosses from left to right and connects to the right atrium (2) (Fig. 8.2.3). The eustachian valve appears as a linear structure crossing the right atrial cavity. Injection
of a solution in a peripheral vein opacifies the right-sided atrial cavity.
of a solution in a peripheral vein opacifies the right-sided atrial cavity.
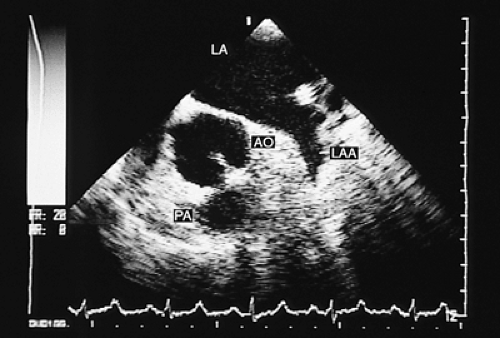 FIGURE 8.2.4. Situs solitus. Transverse plane view at the atrial level. The normal morphology of the left atrial appendage (LAA) can be identified. AO, aorta; LA, left atrium; PA, pulmonary artery. |
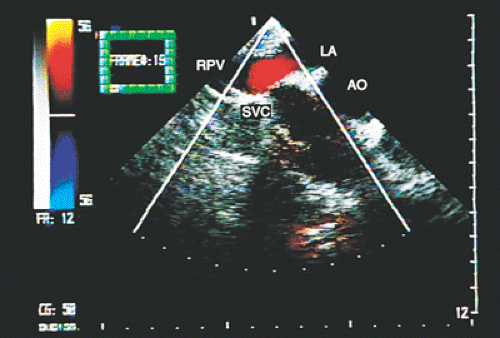 FIGURE 8.2.5. Situs solitus. Atrial situs solitus, showing connection of the right pulmonary vein (RPV) with the left atrium (LA). The superior vena cava (SVC) drains into the right atrium. AO, aorta. |
The left atrial appendage can be identified with recordings in transverse and longitudinal planes by its finger-shaped form with a narrow base (Fig. 8.2.4). This last finding may disappear with volume overload of the atrial cavity.
The pulmonary veins are connected to the atrium situated on the left. With color Doppler their flow is coded in red (Figs. 8.2.5 and 8.2.6) because the flow is directed posteriorly and forward in relation to the transducer.
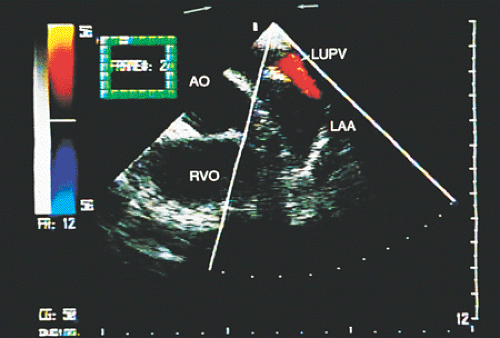 FIGURE 8.2.6. Situs solitus. Transverse plane imaging with color Doppler demonstrates the left upper pulmonary vein (LUPV) behind the left atrial appendage (LAA) and its connection with the left atrium. AO, aorta; RVO, right ventricular outflow. |
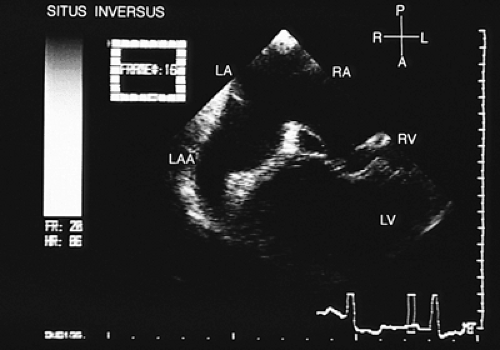 FIGURE 8.2.7. Atrial situs inversus. The anatomically left atrial appendage (LAA) is located on the right. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. |
Situs Inversus
In situs inversus, the right-sided appendage has the characteristics of an anatomically left appendage (Fig. 8.2.7), whereas the left-sided appendage has the characteristics of an anatomically right appendage (Fig. 8.2.8). The atrial cavity on the right is connected to the pulmonary veins (Fig. 8.2.9), whereas the atrial cavity on the left is connected to the venae cavae and receives the coronary sinus. When contrast studies are performed, the atrial chamber situated on the left is opacified (Fig. 8.2.10). The eustachian valve can be
recognized in the atrium situated on the left (Fig. 8.2.11). The connection of the suprahepatic veins to the inferior vena cava and its drainage into the atrium situated on the left can be observed in transgastric recordings (Fig. 8.2.12).
recognized in the atrium situated on the left (Fig. 8.2.11). The connection of the suprahepatic veins to the inferior vena cava and its drainage into the atrium situated on the left can be observed in transgastric recordings (Fig. 8.2.12).
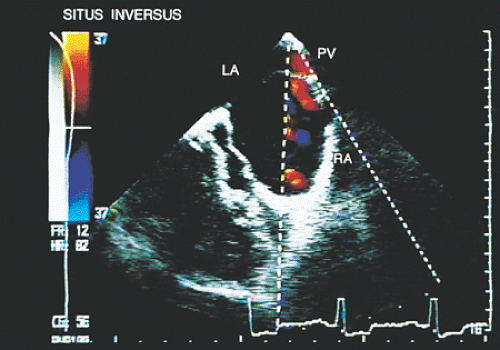 FIGURE 8.2.8. Atrial situs inversus. The presence of atrial situs inversus is demonstrated by the anatomically right atrial appendage (RA) located on the left. The pulmonary veins (PV) drain into the left atrium (LA) found on the right. RA, right atrium. |
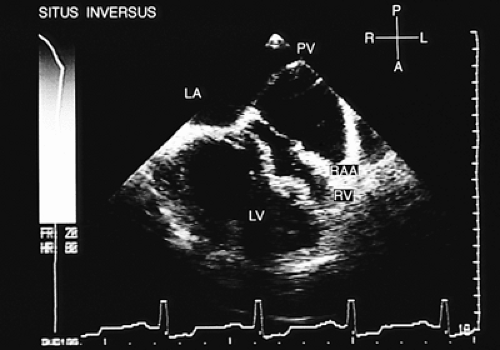 FIGURE 8.2.9. Atrial situs inversus. Transverse plane imaging with color-coded Doppler. The left pulmonary veins (PV) drain into the left atrium (LA), located on the right. LV, left ventricle; RAA, right atrial appendage; RV, right ventricle. |
Findings provided for identifying atrial situs should complement the information obtained from conventional transthoracic and abdominal recordings. These findings can be completed with transgastric recordings; rotation of the transducer directing the beam posteriorly allows evaluation of the position of the inferior vena cava and aorta in relation to the spinal column. In situs solitus the inferior vena cava is found to the right of the column and the aorta to the left. The aorta can be recognized by its pulsations, and Doppler recordings show systolic flow. The flow in the inferior vena cava is both systolic and diastolic and of lower velocity.
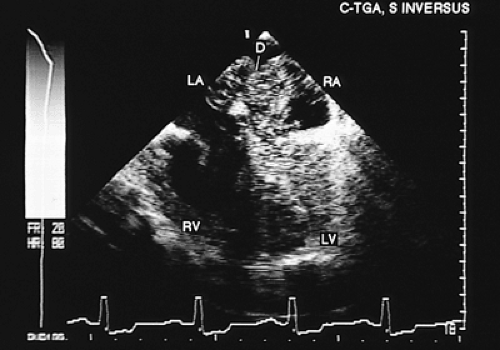 FIGURE 8.2.10. Situs inversus and atrioventricular discordance. A contrast study shows the microbubbles first reaching the right atrium (RA) located on the left, then crossing an interatrial septal defect (D) into the left atrium (LA) and left ventricle (LV). RV, right ventricle. |
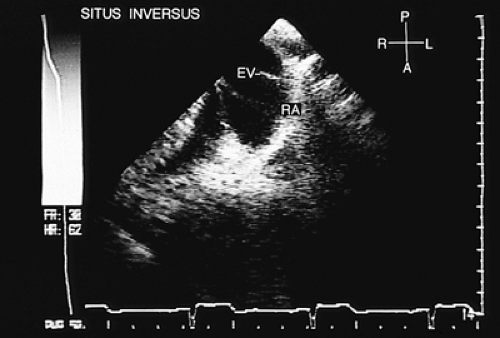 FIGURE 8.2.11. Situs inversus. The right atrium (RA), situated on the left, is identified by the presence of the eustachian valve (EV) |
Following the course of the inferior vena cava in longitudinal sections, its connection with the hepatic veins can be identified, as can its drainage into the right atrium.
In situs inversus a mirror image appears, with the inferior vena cava to the left of the spine and the aorta to the right.
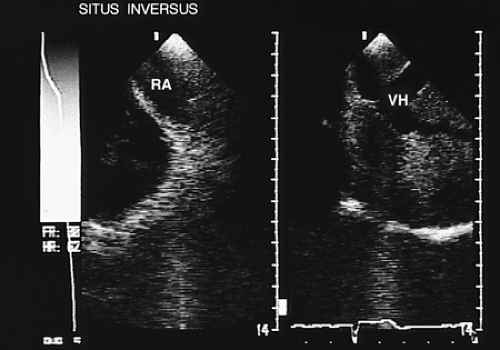 FIGURE 8.2.12. Atrial situs inversus. Situs inversus with progressively superior imaging in the transverse plane. The connection of the hepatic veins (VH) to the left-sided inferior vena cava and right atrium (RA) can be demonstrated in this patient. |
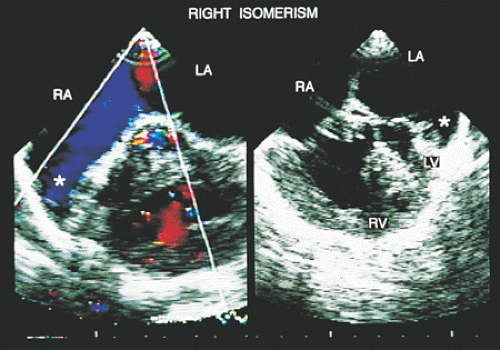 FIGURE 8.2.13. Right atrial isomerism. Transverse plane images. Both atrial appendages (2.13) have a right morphology. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. |
Atrial Isomerism
The term atrial isomerism refers to the absence of anatomic lateralization of the atria, which confers ambiguous characteristics on atrial situs. In right isomerism, transesophageal recordings show that both atrial appendages are of right morphology, that is, they are triangular with broad bases (Fig. 8.2.13). In left isomerism, both atrial appendages are elongated with narrow implantations into their atrial cavities (Fig. 8.2.14).
When atrial isomerism occurs, alterations of systemic and pulmonary venous return often coexist. Because of the important implications such anomalies may have for determining surgical approach, the patterns of venous connection to the heart must be defined before surgical correction.
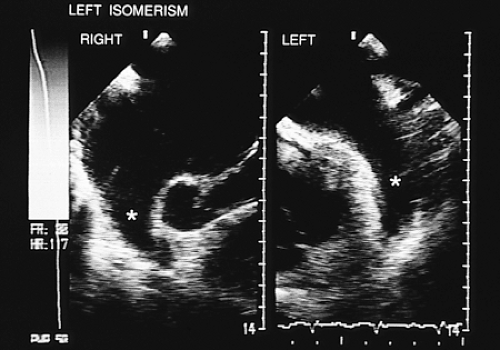 FIGURE 8.2.14. Left atrial isomerism. Transverse plane images. Both atrial appendages (2.14) have a left morphology. |
Although the alterations vary, when a patient presents with right isomerism, it is necessary to check for two superior venae cavae draining directly into both atrial cavities, abnormal connections of hepatic veins to the inferior vena cava, and abnormalities in the pulmonary venous connections, among other anomalies. When left isomerism is present, it is common to find an interrupted inferior vena cava with azygos or hemiazygos continuation, bilateral superior venae cavae, and pulmonary venous return with two veins connected to the atrium located on the right and two to the atrium on the left (2).
Because of the proximity of the transesophageal transducer to the sites of venous return and to the atrial chambers, this technique using the standard transverse axis scan planes may permit a more accurate evaluation of these cardiac structures than is obtained by the transthoracic approach.
The existence of a left persistent superior vena cava can be documented by high left atrial views; the course of the vessel running anterior to the left pulmonary artery and interposed between the left-sided pulmonary veins and left-sided atrial appendage and draining into the roof of the left-sided atrium or connected to the coronary sinus is demonstrated by combining cross-sectional imaging and color flow mapping (Fig. 8.2.15).
The azygos and hemiazygos veins can be demonstrated only in cases in which these vessels are dilated. An azygos vein is sought by combined two-dimensional images and color Doppler posterior and to the right of the right atrium and the right pulmonary artery. The hemiazygos vein is sought posterior to the left atrium and next to the descending aorta (2).
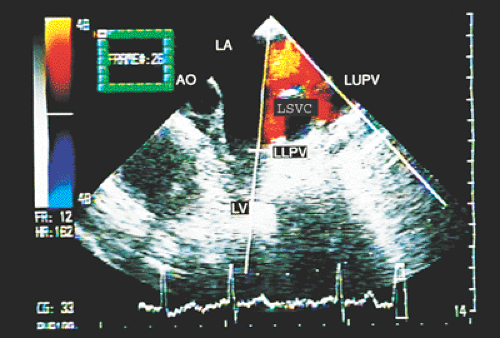 FIGURE 8.2.15. Left isomerism. Left persistent superior vena cava (LSVC) is demonstrated in transverse plane image. AO, aorta; LA, left atrium; LLPV, left lower pulmonary vein; LUPV, left upper pulmonary vein; LV, left ventricle. |
Images similar to those observed with the transducer in subcostal position at the level of the tenth thoracic vertebra can be obtained with transgastric recordings. Right isomerism is diagnosed by visualizing the aorta and the inferior vena cava on the same side of the spine (aortocaval juxtaposition). In this condition, the inferior vena cava is anterolateral in relation to the aorta.
When levoisomerism is present, transesophageal recording makes it possible to document the interruption of the inferior vena cava, an abnormality that occurs in 85% of the cases. In addition, total anomalous connection of hepatic veins can be established and, as described earlier, the azygos and hemiazygos veins can be visualized.
Abnormalities of the right superior vena cava such as its absence or anomalous connection can also be demonstrated with transesophageal recordings. The use of the longitudinal plane in biplane imaging offers substantial additional value in the evaluation of systemic venous connections. However, it contributes little to the assessment of pulmonary venous connections, which are discussed in the section on shunts later in this chapter.
Juxtaposed Atrial Appendages
Juxtaposition is an uncommon malformation in which the two atrial appendages are located on the same side of the great vessels. Left juxtaposition is six times more frequent than the right-sided one and is usually associated with discordant V–A connection, which may be isolated or may be combined with the absence of right A–V connection. The identification of this malformation is important, particularly when a procedure such as a Rashkind septostomy or a Mustard, Senning, or Fontan-type surgery is planned.
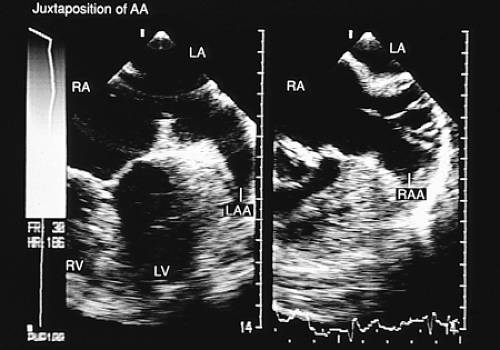 FIGURE 8.2.16. Juxtaposition of atrial appendages. Transverse plane imaging shows both atrial appendages (LAA, RAA) located on the left side. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. |
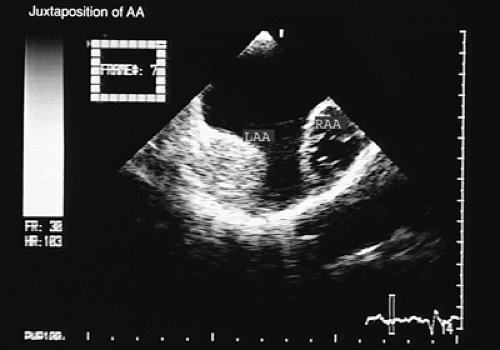 FIGURE 8.2.17. Juxtaposition of atrial appendages. The right atrial appendage (RAA) is imaged more anteriorly as compared to the left atrial appendage (LAA) |
Recognition of juxtaposition with transthoracic echocardiography can be difficult in older children or patients with poor acoustic windows. Its angiographic identification requires an intense contrast in both atria and the juxtaposed atrial appendages. Transesophageal echocardiography is considered the technique of choice for identifying this anomaly. The transesophageal features of left juxtaposition of the atrial appendage include (a) right lateral deviation of the inferior and posterior portion of the atrial septum; (b) a more frontal orientation of the anterosuperior part of the atrial septum, forming the floor and the posterior wall of the junction of the right-sided atrial appendage with the venous component of the atrial cavity (Fig. 8.2.16); (c) the two atrial appendages, each with its own morphology, visualized on the same side, either in superior–inferior positions or side-to-side (Figs. 8.2.16 and 8.2.17); and (d) the association of one or various septal defects of the ostium secundum type, which may be difficult to recognize. The abnormal orientation of the atrial septum may give the false impression of an atrial septal defect located at the site of the junction of the atrial appendage with the venous cavity (3).
Right Atrial Embryonic Remnants
At the third month of embryonic life, the right valve of the sinus venosus divides the right atrium almost completely into two chambers. The sinus portion receives the vena cava and the coronary sinus, and the primitive atrial portion, which is muscular, is associated with the tricuspid valve and includes the right atrial appendage. The embryonic structure undergoes involution between the 9th and 15th weeks of gestation, and its remnants persist as the eustachian and thebesian valves, related to
the orifices of the inferior vena cava and the coronary sinus. Persistence of the right valve of the sinus venosus can vary from a small atrial septation by a membranous remnant of the eustachian valve (Fig. 8.2.18), an area of interconnected trabeculae corresponding to the Chiari network (Fig. 8.2.19) or a complete septation of the right atrium, or cor triatriatum dexter (Fig. 8.2.20). The persistence of remnants of the right valve of the sinus venosus in adulthood has clinical relevance. It has been associated with catheter entrapment, supraventricular arrhythmias, and arterial embolic events.
the orifices of the inferior vena cava and the coronary sinus. Persistence of the right valve of the sinus venosus can vary from a small atrial septation by a membranous remnant of the eustachian valve (Fig. 8.2.18), an area of interconnected trabeculae corresponding to the Chiari network (Fig. 8.2.19) or a complete septation of the right atrium, or cor triatriatum dexter (Fig. 8.2.20). The persistence of remnants of the right valve of the sinus venosus in adulthood has clinical relevance. It has been associated with catheter entrapment, supraventricular arrhythmias, and arterial embolic events.
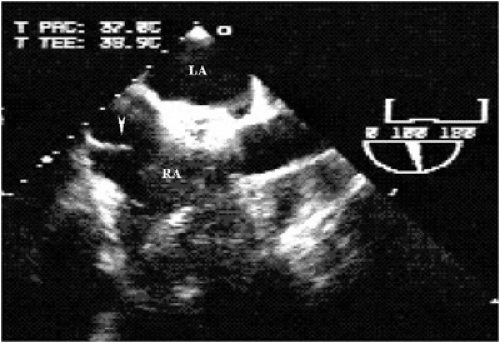 FIGURE 8.2.18. The arrowhead points to a prominent eustachian valve seen as a linear echo in a patient with Amplatzer device closure of an atrial septal defect. LA, left atrium; RA, right atrium. |
Noninvasive diagnosis of the persistence of the right valve of sinus venosus can have limitations when only chest wall images are used. Transesophageal echocardiography defines the characteristics of different embryonic remnants with precision and is useful in differentiating them from thrombi or intracardiac tumors (Fig. 8.2.21).
Ventricular Identification
In transesophageal recordings the right ventricle is recognized by a number of features. A more apical insertion of the tricuspid septal leaflet in the interventricular septum than that of the mitral septal leaflet is present (Fig. 8.2.22). When a perimembranous ventricular septal defect with posterior extension is present, the two A–V valves are inserted at the same level. A muscular structure known as the moderator band can be observed in the inferior portion of the ventricular cavity. The tricuspid subvalvular apparatus has insertions into the interventricular septum (inlet septum) (Fig. 8.2.23). These three characteristics can be identified in the four-chamber transesophageal image.
In transverse transgastric images the two ventricles can be visualized, showing the left ventricle with two papillary muscles and a circular shape and the right ventricle with a crescent-moon shape and muscular trabeculations (Fig. 8.2.24). These recordings are also useful for identifying rudimentary chambers, which is not always possible with transesophageal imaging.
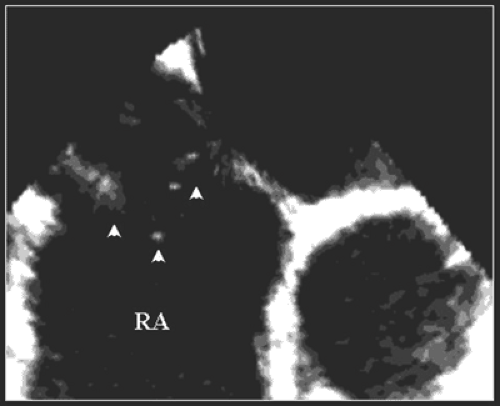 FIGURE 8.2.19. Transesophageal image showing a filamentous structure (arrowheads) extending into the right atrium (RA) |
The presence of the infundibulum in the right ventricle and the fibrous continuity between the mitral valve (left ventricle) and the semilunar valve are other criteria in ventricular identification that can be seen with biplanar transesophageal recordings. Their discriminatory value is lost in congenital heart disease with bilateral infundibulum.
Atrioventricular Connection
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


