A man with severe rheumatic trivalvular disease was treated with surgical implantation of mechanical aortic and mitral prostheses at the age of 30 years and tricuspid bioprosthesis at the age of 50 years. At 61 years of age, he developed severe symptomatic tricuspid regurgitation due to bioprosthesis degeneration and was judged at very high risk for a third surgical approach. The investigators describe the successful transfemoral positioning of a 29-mm Edwards SAPIEN XT percutaneous valve inside the degenerated tricuspid prosthesis, with excellent acute results and no major complications. In conclusion, percutaneous valve-in-valve treatment of degenerated bioprostheses is feasible by the transfemoral route and may be of assistance in very selected patients at high surgical risk.
Case Description
A 62-year-old man with a history of acute articular rheumatism in childhood and previous repeated valvular surgery was referred for recurrent worsening of right-sided heart failure. At the age of 30 years, he had undergone aortic and mitral valve replacement with an Omniscience mechanical prosthesis. In 2001, at 50 years of age, he developed severe tricuspid regurgitation that prompted surgical replacement with a PERIMOUNT Magna 31-mm prosthesis (Edwards Lifesciences, Irvine, California). In the following years, despite receiving long-term oral anticoagulation, he developed chronic obstructive pulmonary disease requiring oxygen therapy and symptomatic recurrent transient cerebral ischemic attacks associated with permanent atrial fibrillation.
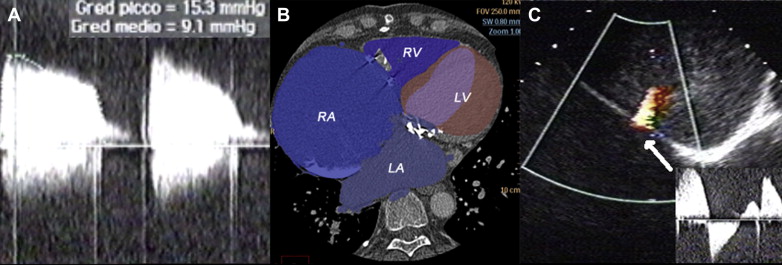
In 2012, when the patient was 61 years old and experiencing worsening fatigue and anasarca, severe stenosis of the tricuspid bioprosthesis was apparent (transthoracic echocardiographic transvalvular gradient 15 mm Hg, mean 9 mm Hg, estimated area <0.5 cm 2 ; Figure 1 ). The left and right atria were severely enlarged (left and right atrial volumes 1,275 and 1,300 ml, respectively; Figure 1 ), and a large right-to-left shunt was detected through a widely patent foramen ovale ( Figure 1 ). The left ventricular ejection fraction was 65%. Right ventricular contractility was normal.
Given the high risk of a third operation and the possibility of needing further reintervention to replace the mechanical valves in the near future, transcatheter valve implantation was performed. A few cases of similar procedures have been reported in patients with single-valve disease by the transjugular, transfemoral, or transatrial approach.
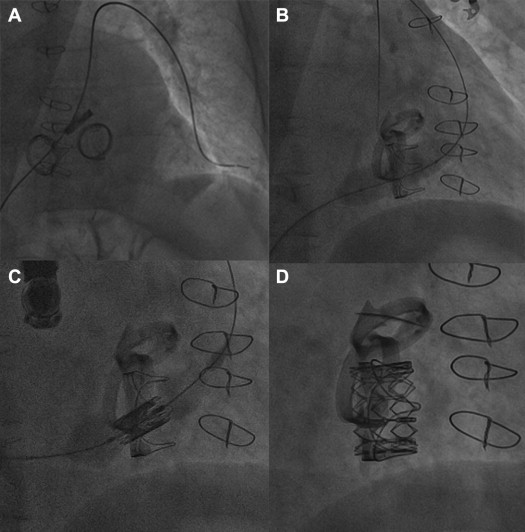
Under general anesthesia and mechanical ventilation, the common right femoral vein was percutaneously cannulated and progressively prepared with 16Fr to 22Fr dilators before uncomplicated advancement of a 20Fr Edwards introducer over an extra-stiff guidewire. The tricuspid valve was crossed with a pigtail catheter and the same extra-stiff wire after several attempts because of severe right atrial enlargement. A Simmons-2 hydrophilic catheter was advanced over a regular wire into the left main pulmonary artery as distally as possible to advance the extra-stiff wire for optimal support ( Figure 2 ; Supplemental Video S3 ). Careful bioprosthesis predilatation was performed with 25- and 28-mm-diameter balloons inflated at nominal volumes ( Figure 2 ; Supplemental Video S4 ). After reverse mounting on the NovaFlex system (Edwards Lifesciences) for adapting to the tricuspid position and 180° rotation of the delivery to achieve correct flexibility toward the atrioventricular valve, a 29-mm Edwards SAPIEN XT bioprosthesis was advanced into the inferior vena cava and correctly aligned with its balloon. A right anterior oblique 50° projection allowed precise valve-in-valve positioning of the prosthesis ( Figure 2 ), which was then cautiously inflated at nominal volume to correct minimal shifts without need for rapid pacing because of the relatively low right-sided pressures ( Supplemental Video S5 ). Excellent acute angiographic ( Figure 2 ) and echocardiographic results were achieved (postprocedural mean gradient 3 mm Hg), with rapid reversal of the right-to-left shunt through the patent foramen ovale ( Figure 3 ; Supplemental Video S2 ). The patient was discharged after an uneventful 7-day stay.