28
Traditional urban pollution
The twentieth century was marked by a rapid increase in industrial processes involving consumption of fossil fuels, particularly in the years following the Second World War. The pollutants generated by coal-fired power plants, steel mills, smelters and fertilizer plants became increasingly prevalent in the ambient air of developed regions of the world, particularly Europe and the USA. Even before the Second World War, air pollution was becoming an increasingly recognized reality. The first health crisis directly attributable to air pollution occurred in the Meuse Valley in Belgium in December 1930, where hundreds became ill and approximately 60 people (10 times the mortality rate) died during a 3 day period. The cause of this episode was a perfect combination of geography, weather and heavy industrial activity that resulted in a stagnant air mass containing high concentrations of toxic pollutants that settled over the towns of Huy and Liege. In the USA, a cloud of smog was visible over the Los Angeles skyline by the mid 1940s, and the coal-fueled Midwestern industrial boom filled the skies of the populous Eastern seaboard with airborne pollutants. A weather pattern similar to that seen in the Meuse valley occurred over the small town of Donora, Pennsylvania in 1948, once again concentrating the pollutants from nearby factories and causing widespread respiratory symptoms and 20 deaths (6 times the mortality rate).
Although both the events in Liege and Donora received intense political and media attention in their respective countries at the time of each occurrence, the event that probably receives the most attention in environmental health literature is the London Fog of December 1952. During a four day period of December 1952, a dense, pollutantladen fog settled over the city and was blamed for about 3000 excessive deaths during the following weeks. Recent investigators have applied more contemporary modeling techniques to public health records from the period and have raised the estimated death toll to as many as 12,000 excess deaths. Even taking the historical figure of 3000 deaths, the astounding number of deaths from this episode is considered by many to be the first major stimulus to the study and reduction of air pollution. Despite the many lessons learned from these historic environmental disasters, the rapidly developing countries of Asia, the Middle East and Latin America will probably suffer similar episodes given their large reliance on traditional energy sources and industrial practices to build their economies. In today’s global society, countries that have already learned from such disasters should help develop methods of industry that allow for sustainable growth, without a return to the smoggy days of London, Liege and Donora. The following will include a description of the major components of traditional sources of air pollution, a current understanding of the health effects of each component, and a brief summary of current policy issues. Common patient questions are addressed below (Table 28.1).
Table 28.1 Selected issues for patients with respiratory disease
| Question | Answer |
| When is the best time to exercise outdoors? | In cities, air pollution from ozone is generally lowest early mornings before rush-hour traffic, so exercise at that time, not close to a highway |
| How can exposure to air pollution be minimized? | At a population level, by legislation to reduce air pollutants At a personal level, reduce use of gasoline or diesel, and limit outdoor activities during high pollution episodes |
| How can the effects of air pollution on asthma exacerbations be prevented? | By reducing outdoor exposure, by reducing exposure to relevant allergens and other asthma triggers and by optimizing asthma control with prescribed medications |
| Should a patient with lung disease avoid living in a city? | Ozone concentrations can also be high in rural areas with natural sources of NOx contributing to ozone in the summer months. No studies to date have shown overall improved outcomes among those who have moved to rural areas For patients with cardiovascular disease or COPD, there also is no current evidence to support a move to a more rural setting which may have less air pollution but also may have less availability of healthcare resources |
| Should outdoor play be restricted for children in cities? | The generally relatively small risks of air pollution effects need to be balanced against the known beneficial effects of exercise for children, and there are currently no recommendations to restrict outdoor exercise for children except at times of extreme air pollution episodes |
| How much COPD can be blamed on outdoor air pollution? | The answer to this remains unclear but smoking, cooking with biomass fuel and occupational exposures remain the most important causes of COPD |
Particulate matter (PM) includes air particles from many different sources and of various sizes. Total suspended particles are composed of particles up to 40 μm in diameter. PM10 refers to particles up to 10 μm in diameter and are those which can be inhaled past the upper airways. PM is further delineated into PM10-2.5 and PM2.5, the latter of which are fine particles up to 2.5 μm in diameter. Ultrafine particles are those which have a diameter less than 0.1 mm. Other important characteristics of PM are the contributing source and its various components. PM can be directly produced by combustive sources such as coal-fired power plants, or can be formed in the atmosphere as a result of the combination of gases from motor vehicles, industries and natural sources. Direct sources of PM in the traditional urban environment include coal- and oil-fired power plants and industry. The actual composition of PM2.5 varies tremendously based on both region and season. In a study of composition of PM2.5 over 187 counties in the USA, only seven of the 52 compounds analyzed accounted for 1% or more of the yearly or seasonal average of total PM2.5 mass. These included ammonium, elemental carbon, organic carbon matter, nitrate, sodium, silicon and sulfates and made up 79-85% of the total PM2.5 mass. PM and its effects vary based on source, region and season, which are also linked to particle size and composition.
Many efforts to develop a simple and consistent animal model of particle induced health effects have been made with variable success. The development of techniques to concentrate ambient particles at both New York University and Harvard School of Public Health in the 1990s has made standardized exposures easier to achieve, and have advanced this line of research immeasurably. These techniques allow investigators to collect ambient air and concentrate the particles without necessarily altering the distribution of sizes and chemical composition of the pollutants. Results of experiments employing materials obtained via these concentrators in closed chamber animal experiments follow.
Effects on the respiratory system
Early experiments compared normal rats with those exposed to 250 ppm SO2/day for 6 weeks as a method of inducing chronic bronchitis. The rats were then exposed to either concentrated ambient particles (CAPs) or filtered air 5 hours per day for three consecutive days and assessed for measures of pulmonary function and inflammation. The ambient air particle mass on each day was 7.1, 19.1 and 18.6 μg/m3 and after concentration via the Harvard/EPA Ambient Particle Concentrator levels of 205.5, 733.3 and 606.7 μg/m3 were achieved in the exposure chamber. After exposure, the chronic bronchitis rats interestingly had significant increases in both tidal volume and peak expiratory flow, whereas normal rats had increased tidal volume over baseline. Bronchoalveloar lavage showed no difference in total cell counts, but a shift in the cellular differential towards neutrophilic inflammation and increased fluid protein content was observed. Similar experiments in normal dogs showed no statistically significant differences in bronchoalveloar lavage cellularity, but a nonsignificant trend towards increased neutrophils. Exposure to CAPs, collected from a community in southwestern Detroit with known high levels of air pollution showed no demonstrable airway inflammation in healthy rats; however, ovalbumin-sensitized rats did have significant, although variable inflammatory responses after five consecutive days of exposure. Finally, no differences were found in pulmonary immune responses in rats exposed to CAPs collected in New York City; however, there was a significant elevation in blood polymorphonuclear leukocytes.
Effects on the cardiovascular system
Acute exposure (4 weeks) to PM10 has been shown to enhance progression of atherosclerotic lesions in rabbits with inherited hyperlipidemia. A longer term (6 month) study of apolipoprotein E knockout mice (ApoE -/-) who were exposed to concentrated PM2.5 for 6 hours per day, 5 days per week also showed increased atherosclerosis, particularly when fed a high-fat diet. These mice were also found to have alterations in vasomotor tone, heart-rate fluctuation and vascular inflammation. These effects also seem to translate into worse clinical outcomes in models of myocardial infarction, as dogs exposed to CAPs developed a significantly greater degree of ST segment elevation after coronary artery occlusion.
28.2.3 Health effects of PM in humans
Short-term health effects of PM
The influence of particulate air pollution on short-term health effects has been largely examined through time-series studies, which generally relate daily PM levels to various indicators of disease. Several multi-city, time-series studies have been performed, including a 90-city study in the USA, the National Morbidity, Mortality and Air Pollution Study (NMMAPS). In this study, multiple pollutants were examined and PM10 levels were found to be associated with an increase in mortality, with the largest effect size seen in the northeast region. Nationally, for every 10 μg/m3 increase in PM10, a 0.2% increase in mortality with a 1-day lag was detected. In addition, there was a 0.3% increase in cardiopulmonary-specific mortality, for every 10 μg/m3 rise in PM10. Hospital admissions for cardiovascular disease and COPD among elderly in 14 cities from NMMAPS were also correlated with PM10 levels.
The multi-city European project, APHEA (Air Pollution and Health: a European Approach), has also studied the short-term effects of particulate air pollution. In the initial study, black smoke (representing PM < 4 μm) and PM10 were correlated with daily mortality in 12 European cities. A 50 μm3 increase in black smoke and PM10 was associated with respective 3 and 2% rises in mortality in western European cities. A more comprehensive study, APHEA2, included 29 European cities and measured health outcome and particulate levels over 5 years, beginning in 1990. Similar to NMMAPS, APHEA2 correlated a 0.6% increase in daily mortality with a 10 μg/m3 rise in PM10 and black smoke. Larger effects sizes were noted among elderly, and in cities with higher NO2 and warmer climates.
Long-term health effects of PM
Health effects of chronic air pollution in traditional urban areas were investigated in a study comparing three counties in Utah, each with a major city. Two of the counties, Utah and Cache Counties, were similar, in terms of demographics, religion and minimal tobacco use, until a steel mill was built in Provo (Utah County) in the 1940s. Salt Lake County, which included the third city, was notably more characteristic of a US city. Smoking, for example, was twice as common in Salt Lake County. Approximately 45% of PM10 levels in Utah County were produced by the Provo steel mill. From 1960 to 1970, respiratory cancer death rates doubled in Utah County, in contrast to Cache County, where they were relatively unchanged, and continued to increase in subsequent decades. Long-term air pollution, which increased substantially in Provo and was largely attributed to the steel mill, was associated with increased mortality and morbidity from both respiratory cancers and nonmalignant pulmonary disease. Temporary cessation of operations at the Utah County steel mill in 1986 led to decreased PM10 levels, and was associated with fewer county-wide hospital admissions for respiratory illnesses [1].
Fine particulate matter and mortality
More specific health effects of fine particulate matter have also been studied. The effects of long-term air pollution and PM2.5 were studied in the cohort from the Harvard Six Cities Study, which included roughly 8100 adults from Watertown, MA, Harriman and Kingston, TN, St Louis, MO, Steubenville, OH, Portage, WI and Topeka, KS, areas with differing degrees of air pollution. Central air pollution and individual health data were collected from the mid-1970s to 1991. Overall mortality in this cohort study was most strongly linked with fine (PM2.5), inhalable particulate matter, especially sulfates, with relative rate ratios of 1.26-1.27 across the range of pollution found in these cities. Specific causes of death linked to air pollution in this study included lung cancer and cardio-respiratory illness [2].
An association between PM2.5 and mortality was also found as part of the Cancer Prevention Study II, where data on 1.2 million people across the USA was prospectively collected. Overall, PM2.5 levels decreased in the USA from 1979 to 2000, which was the span over which air pollution data was collected. Whether assessed at the start or end of the study, air pollution as reflected by PM2.5 levels was linked with all-cause, cardiorespiratory and lung cancer deaths. For a 10 μg/m3 increase in PM2.5, there was a relative risk of 1.06 (95% CI 1.02-1.11), 1.09 (95% CI 1.03-1.16) and 1.14 (95% CI 1.04-1.23) for all-cause, cardio-pulmonary and lung cancer mortality, respectively [3].
In a follow-up study of the Harvard Six Cities cohort, all-cause, cardiopulmonary and lung cancer mortality were again found to parallel PM2.5 levels [4]. As seen in CPSII, PM2.5 levels decreased in all six cities, with greatest reduction in the most polluted cities. For every 10 mg/m3 decrease in PM2.5 seen in the follow-up period, there was a reduction in all-cause mortality (RR = 0.73; 95% CI 0.57-0.95). This was seen for cardio-respiratory mortality, but not for lung cancer deaths. This follow-up study reiterated the association between PM2.5 levels and mortality, and also suggests that health effects of air pollution can be attenuated [4].
Fine particulate matter and morbidity
PM2.5 has also been studied in terms of morbidity among both adults and children. Hospital admissions in a Medicare population were recently reviewed in conjunction with available PM2.5 levels in 204 US counties to examine the short-term effects of air pollution on cardiopulmonary morbidity. Daily variations in PM2.5 were linked to change in hospital admission rates for heart failure, COPD, respiratory tract infections, cerebrovascular disease, peripheral vascular disease, ischemic heart disease and heart rhythms. Hospitalization rates for up to 2 days of lag time after the measured PM2.5 level were examined. Cardiovascular hospitalizations were most likely on day 0 (except for ischemic heart disease), whereas there was more variability in timing of hospitalization for respiratory illnesses. For every 10 mg/m3 increase in PM2.5, there was a 1.28% higher risk of same-day hospitalization due to heart failure. The authors calculated that annual admissions for heart failure would drop by 3156, in these 204 counties, if PM2.5 was reduced by 10 mg/m3. Hospitalizations for respiratory tract infections and COPD would be reduced by 2085 and 990, respectively [5]. Some regional variation was also seen, with greater cardiovascular effect size seen in Eastern counties.
Fine PM and cardiovascular morbidity
Cardiovascular health effects include reduced heart rate variability as a risk factor for mortality, especially in elderly subjects. Diminished heart rate variability was linked with higher PM2.5 levels in a small, elderly population in Utah. More recently, a study of the cardiovascular effects of long-term air pollution in a large cohort of postmenopausal women without pre-existing heart disease was published (Women’s Health Initiative Observational Study). An adjusted hazard ratio of 1.24% (95% CI 1.09-1.41) for time to first cardiovascular event, including cerebrovascular events, was associated with a 10 μg/m3 increase in PM2.5. Other pollutants were measured, but were not significantly linked to cardiac morbidity. The strongest findings were for mortality endpoints, and especially for death due to definite coronary heart disease. Higher hazard ratios for mortality endpoints were found than in previous cohort studies which included men, which may reflect greater vulnerability of women in terms of air pollution or differences in methodology of the studies. Theories that have been offered to help explain the effect of air pollution on cardiovascular disease include accelerated atherosclerosis, change in autonomic control and increased inflammation.
Fine PM and respiratory morbidity
Clinical studies assessing the association of PM2.5 on respiratory morbidity have also been performed. Populations with pre-existing illnesses seem to be at greater risk of negative effects of air pollution. In APHEA2, a 10 μg/m3 rise in PM10 levels was correlated with an increase in respiratory admissions, including children and adults with acute asthma and COPD, by approximately 1%. In another study, children with asthma were given personal exposure monitors and followed for 2 week periods. FEV1 (percentage predicted) was found to be negatively associated with the level of personal, fine PM exposure. Nonmobile measurements of PM were also recorded and associated with pulmonary function, but more weakly than personal PM levels. In addition, personal PM had a larger effect in atopic boys with susceptibility to indoor allergens.
Children with more severe asthma also seem to be more susceptible to effects of particulate air pollution, in a study of schoolchildren in Denver, Colorado. PM2.5 levels were found to be highest in the morning hours when children were traveling to school. Higher morning PM2.5 levels resulted in greater use of bronchodilators at school, also suggesting rapid onset of symptoms. This relationship was also more pronounced in children with severe asthma. In addition, urinary leukotriene E4 was measured during the school day and was associated with morning PM2.5 levels. Another personal monitor study in Seattle, Washington examined lung function effects of particulate air pollution in children with asthma and adults with COPD. Decrease in FEV1 was associated with PM2.5 measurement at a central location, after a 1-day lag, in patients with COPD, although it did not correlate with personal levels. In asthmatic children not on antiinflammatory medications, PM2.5 was associated with declines in MMEF, FEV1 and PEF. While some change in lung function was seen overall, the correlation was stronger in asthmatics not on anti-inflammatory medications, lending support to possible PM triggering of inflammatory mechanisms [6]. Elevated exhaled nitric oxide was associated with PM2.5 levels in these same children in an earlier report, further highlighting the potential inflammatory effects of air pollution. While further categorizing the respiratory effects of air pollution, these studies also point out that use of daily averages of PM levels may not be sufficient to fully understand the health effects of particulate air pollution.
Associations between respiratory illness and particulate air pollution have been further strengthened by studies involving experimental exposures to PM in humans, which help define underlying mechanisms for disease causation. In one study, healthy volunteers were exposed to CAPS (concentrated ambient particles 0.1-2.5 μm in size) for 2 hours. Final exposure concentrations ranged from 23.1 to 311.1 μg/m3, and were dependent on variation in outside particulate levels. There were no differences in pulmonary function testing or symptoms between those exposed to CAPS versus filtered air controls. However, increases in cellularity and neutrophil counts of bronchoalveolar lavage fluid were seen after CAPS exposure as compared with filtered air. In addition, bronchoalveolar lavage fluid neutrophils appeared to increase in a dose-dependent manner, highlighting a possible inflammatory pathway of particulate air pollution induced illnesses.
In recent literature, particulate air pollution has been increasingly associated with adverse health effects. As reviewed, there is evidence for both increased mortality and cardio-respiratory morbidity linked to PM exposure. While earlier studies focused on short-term mortality risk, the current body of research supports an increased chance of long-term consequences as well. There has also been focus on highly susceptible populations, such as those with chronic respiratory illnesses as well as the elderly. Work on elucidating the pathogenesis of PM-associated cardiovascular and respiratory morbidity has also progressed. In the USA, the National Ambient Air Quality Standards (NAAQS) for PM were slightly lowered in 2006 on the basis of growing evidence for adverse PM-related health effects. Adverse health outcomes have been seen even at low PM concentrations in recent time-series studies and many argue, in fact, that PM NAAQS are not stringent enough.
28.3.1 Characteristics of sulfur oxides
Sulfur is a major component of fossil fuel sources such as coal and oil, as well as several common metal ores such as iron, zinc, and copper. Combustion of these materials leads to the formation of the gas sulfur dioxide, which may dissolve in water vapor to form acidic aerosols that eventually fall to the earth in the form of acid rain. These acidic byproducts of sulfur combustion primarily concentrate in lakes and streams, often resulting in a decrease in pH significant enough to reduce, or in some cases eliminate natural aquatic wildlife populations. Sulfur dioxide may also combine with other particles in the air to form sulfate particulate matter, which contributes to visual pollution, particularly in summer months when it forms a milky, white haze in the afternoon. While ambient SO2 concentrations are highest close to the source of production (coal-fired power plants, petroleum refineries, smelters), sulfate particles can have an impact relatively far away since their small size lends to long distance transport. Intercontinental transport of SO2 and other toxic emissions promises to be an important policy issue for years to come.
Sulfur dioxide is rapidly absorbed by mucosal surfaces of the nasopharynx and upper airway. It is readily soluble in epithelial lining fluid, forming acidic species that result in cellular damage. Although this rapid upper airway absorption protects the lower airways from the irritant effect, the increase in minute ventilation and tidal volume during exercise overcomes its absorptive capacity, often resulting in lower airway effects. Acute exposure to sulfur dioxide can result in a variety of symptoms, most commonly dyspnea, cough, and exacerbation of chronic cardio-pulmonary disease. Controlled chamber experiments, which allow for measurements of the specific effects of SO2, have demonstrated a spectrum of responses in healthy individuals, from no effect to marked bronchoconstriction. The asthmatic population is generally more susceptible, but in these controlled settings without the additive effects of other pollutants, the effects are generally reversible in minutes to hours. The minimum concentration required to demonstrate a decline in lung function in normal is approximately 1000 ppb (2860 μg/m3), whereas asthmatics may have significant reductions in lung function at as low as 400 ppb (1144 μg/m3). For reasons mentioned above, the effects of SO2 may be augmented by exercise, and in one study an interaction was found when SO2 was administered with cold dry air.
28.3.3 Effects of chronic exposure
The effects of long-term exposures to SO2 are less clear, and there is controversy in the literature as to its negative effect independent of sulfate and nonsulfate PM. As part of the APHEA project, a 3% increase in daily mortality was shown with an increase in SO2 by 50 μg/m3 (95% CI 2-4%) that was independent of PM10. However, six other studies that resulted from APHEA data failed to replicate these findings. Several Chinese investigators have been able to demonstrate an effect of SO2 on morbidity and mortality independent of total suspended particles in a variety of locations in China, which may reflect a difference in population susceptibility or unique characteristics of industrial emissions in the region. Since PM2.5 may be the more specific causal agent in PMrelated disease, further data on SO2 effects independent of PM2.5 would be valuable in establishing an independent effect. One such analysis of data from Chongqinq, China did show independent increases in relative risk of respiratory and cardiovascular mortality independent of PM2.5. Overall, SO2 should be viewed as an airway irritant with several demonstrated acute, negative effects on respiratory symptoms and physiology, while its long-term effects on morbidity and mortality remain a topic for investigation.
Worldwide sulfur emissions peaked in 1989, and have declined since then, although they remain well above those at the beginning of last century. Initial efforts to decrease the local levels of SO2 involved mandating the construction of tall (in some cases 500 feet high) smokestacks so that SO2 would disperse over a greater area and reduce the effects on the local population. While this policy was successful in reducing the human impact of SO2, the generation of PM remained unabated until policy to decrease the total amount of sulfur emissions produced was enacted. The first Clean Air Act was passed by the UK during the 1950s after recognizing the health impacts of the London Smog, and the USA followed suit in 1963 with subsequent modifications, most notably in 1970 with the establishment of the Environmental Protection Agency (EPA). The most recent revision of the Clean Air Act in 1990 included a specific Acid Rain Program that implemented a ‘cap and trade’ system whereby individual power plants were given an allowance of emissions per unit of energy when compared with a historical standard. If this allowance is then exceeded, additional emissions ‘credits’ may be bought or traded for on the open market. This policy was hailed as an approach to air pollution control that allowed for some flexibility within the industry to reduce emissions without necessarily forcing the immediate closure of older plants that would be costly to update to cleaner technologies. As a result of the initial phase of the Acid Rain Program, SO2 emissions in the USA declined by 17% between 1990 and 1998, and Phase II of the program promises further reductions in years to come. As mentioned previously, concerns about industrialization in Asia and other parts of the developing world temper optimism about a true reduction in sulfur emissions globally, since many of the improvements made in developed countries could easily be nullified by increased emissions worldwide.
28.4.1 Characteristics of nitrogen oxides
Although there are many known sources of nitrogen oxides in rural settings related to nitrogenous fertilizers and manure management, traditional urban sources (excluding vehicular) arise primarily from combustion of fossil fuels such as coal and oil for electricity production, with a lesser contribution by sewage treatment plants. Fossil fuelrelated power generation initially leads to release of nitrogen oxide, which can be further oxidized to nitrogen dioxide in the atmosphere. Nitrogen dioxode is a colorless, odorless gas, whereas nitrogen oxide has an odor and a reddish-brown color that contributes to visible pollution independent of associated particulates. The combination of these and other oxidized nitrogen species are typically referred to as NOx. As will be described in subsequent sections, the primary health effects of NOx species are ozone formation via interactions with volatile organic compounds in the presence of sunlight. In addition, NOx contributes to acid rain along with sulfur oxides, and has effects on water systems independent of pH by upsetting the balance of nutrients required by aquatic plants and animals. This process of excess nitrogen deposition is termed eutrophication, and can result in algae overgrowth that eventually depletes oxygen from the body of water creating a ‘dead’ zone. Nitrous oxide (N2O), a lesser component of NOx, persists in the atmosphere for approximately 120 years and is thought to be a significant contributor to global warming.
In terms of direct health effects of nitrogen oxides, NO2 has widely recognized effects from known occupational exposures (silo-filler’s disease), during which a highly concentrated exposure leads to severe respiratory symptoms and adult respiratory distress syndrome. In the case of ambient pollution, however, studies vary in their ability to demonstrate or refute the specific role of NOx in human disease due to the large populations required and potential confounding from other pollutants. Controlled experiments that simulate levels commonly observed in the atmosphere have shown no effect in healthy subjects at NO2 concentrations up to 0.60 ppm, but asthmatics were demonstrated to have a decrease in FEV1 during exercise and cold air inhalation after exposure to NO2 at 0.30 ppm.
28.4.3 Effects of chronic exposure
Large-scale population based studies are less conclusive, although several are suggestive. A retrospective analysis of hospital asthma admissions in Hong Kong found the relative risk of admission was 1.028 (95% CI 1.021-1.034) for every 10 μg/m3 rise in NO2 concentration Similar findings were obtained in a study that included controls for four types of pollen, as well as the more usual PM, SO2 and ozone. Increases in viral respiratory tract infections have been observed in asthmatic children, and patients over the age of 65, and there is some in-vitro data to suggest altered host response to infection with respiratory syncytial virus. In terms of mortality, although some found no association with increased mortality from NO2 independent of PM, several others found positive associations with statistically significant increases in total mortality 0.30% (95% CI 0.25-0.35%), cardiovascular disease mortality 0.41% (95% CI 0.34-0.49%), and respiratory mortality 0.34% (95%CI 0.17-0.51%) for every 10 μg/m3 increase in NO2 in an analysis of APHEA-2 data [7]. A cohort study of 4800 German women living in North Rhine-Wesphalia found that both total and cardiopulmonary mortality correlated with a rise in the NO2 interquartile range by 16 μg/m3, when adjusted for smoking and socioeconomic status [8].
As in the case of sulfur oxides, levels of nitrogen oxides have been decreasing in the USA and Europe as the result of legislation. Data from the UK National Atmospheric Emissions Inventory show energy generating emissions declined by approximately 45% between 1990 and 2003, and US EPA data show a 30% decline over a similar period. These data do not take into account reductions due to a decrease in industrial activity in developed countries, but also fail to note the impact of increased industrialization in Asia. In summary, nitrogen oxides in concentrations commonly observed in the atmosphere are likely contributors to cardiopulmonary morbidity in susceptible populations; however, definite mortality associations remain to be fully elucidated (Table 28.2).
Table 28.2 Summary of health effects of outdoor air pollutants (dependent on exposure concentrations and susceptibility of population)
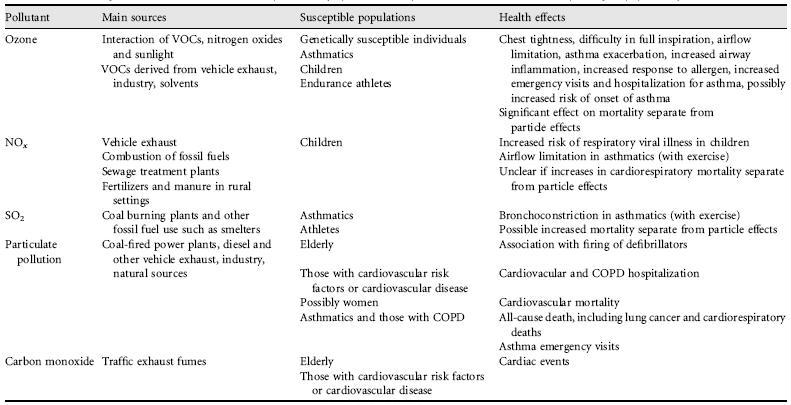
VOC, volatile organic compounds.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


