29 Tissue Doppler Imaging in the Fetus
I. HOW TISSUE DOPPLER WORKS
A. Blood versus tissue velocities
1. One of the new techniques that is being investigated in many centers is myocardial velocities as a way to assess fetal ventricular function. Grouped together, these techniques are jointly known as tissue Doppler.
2. The movements of the myocardium are much slower than the flow of blood into and out of the ventricles.
a. Inflow and outflow velocities in the human fetus are in the range of 0.5 to 1.0 m/s (50-100 cm/s).
b. Myocardial velocities, albeit stronger signals, average about one tenth of these velocities, ranging from 0.05 to 0.1 m/s (5-10 cm/s).
2. These low-velocity signals are complex in their orientation due to the three-dimensional (3-D) nature of ventricular contraction.
B. Heart motion
a. Classically, ventricular function has been described as radial changes in diameter (fractional shortening).
b. Radial change is the difference in the diastolic and systolic dimensions divided by the diastolic dimension.
c. These movements are known as radial changes in dimension and are accompanied by longitudinal ones (base-to-apex changes).
d. Each radial motion is not in just one plane but in two. Thus, the complex spatial movements of the heart require simplification into simple linear movements.
a. The normal movement of the heart is for the base to move downward toward the apex in systole.
b. Following this, the muscle actively relaxes back upward in a biphasic pattern of early and late diastolic movements.
c. These are analogous to the biphasic nature of the velocities of ventricular inflow, the E and A waves of early and late diastole.
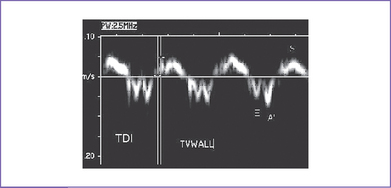
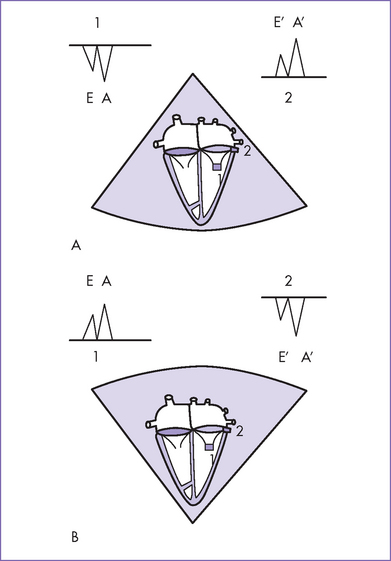
d. E and A waves in the fetus always have a pattern such that the A wave is larger than the E wave (Fig. 29-1).
e. It is intriguing to find that the longitudinal myocardial tissue Doppler velocities in the fetus are similar to the E’ wave or early diastolic relaxation velocity, being smaller than the later diastolic A’ velocity (Fig. 29-2).