Thymic Neuroendocrine Carcinomas/Tumors
Borislav A. Alexiev, M.D.
Anja C. Roden, M.D.
Allen P. Burke, M.D.
The histopathologic classification of primary neuroendocrine tumors (NETs) of the mediastinum is similar to that of NETs of other organs. There are two classifications. One follows that of the lung (carcinoid, atypical carcinoid, large cell neuroendocrine carcinoma, and small cell carcinoma).1 The other is similar to that used in the gastrointestinal tract (well-differentiated NET/carcinoma, moderately differentiated neuroendocrine carcinoma, and poorly differentiated neuroendocrine carcinoma).2 There are advantages to both systems. The rationale for considering all these tumors as carcinomas is the observation that all mediastinal carcinoids bear a significant risk for recurrence, metastasis, and tumor-associated death. However, carcinoids are treated far differently from small cell carcinoma, which is a clinically distinct entity. Not all small cell carcinomas show demonstrable neuroendocrine differentiation, which may justify a category for them separate from large cell neuroendocrine carcinoma (see Chapter 85, Section 1).
Terminology
Thymic epithelial tumors that are predominantly or exclusively composed of neuroendocrine cells are classified as neuroendocrine carcinomas of the thymus. They have to be distinguished (1) from otherwise typical thymic carcinomas, which may contain scattered or groups of neuroendocrine cells, and (2) from nonepithelial neurogenic tumors, particularly paragangliomas.1
Typical (classic) carcinoid (well-differentiated NET/NEC, low grade) is a well-differentiated NET composed of polygonal cells with granular cytoplasm arranged in ribbons, festoons, solid nests, and rosette-like glands. Tumors have <2 mitoses per 10 HPF, and necrosis is absent.
Atypical carcinoid (well-differentiated NET/NEC, intermediate grade) is defined as a well-differentiated NET with (1) mitotic rate of 2 to 10 per 10 HPFs and/or (2) necrosis.
Large-cell neuroendocrine carcinoma (poorly differentiated NET/NEC, high grade): A high-grade thymic tumor composed of large cells with neuroendocrine morphology such as palisading, trabeculae, nesting, or rosette-like features; necrosis that is usually extensive; a high mitotic rate (mitotic rate of >10 per 10 HPF); and either neurosecretory granules by electron microscopy or positive neuroendocrine immunohistochemical markers.
Small cell carcinoma, neuroendocrine type (poorly differentiated NET/NEC, high grade) is a high-grade thymic tumor consisting of small cells (<3 lymphocytes) with scant cytoplasm, ill-defined cell borders, finely granular nuclear chromatin, and absent or inconspicuous nucleoli. The cells are round, oval, or spindle shaped, and nuclear molding and crush artifact with nuclear streaming and incrustation of vessels is prominent. High mitotic rate, apoptotic bodies, and large areas of geographic necrosis are typical. A variant is a combined small cell carcinoma with squamous cell carcinoma or adenocarcinoma.
Incidence and Clinical Presentation
Primary thymic neuroendocrine carcinomas are rare and account for no more than 5% of all mediastinal tumors.3 Thymic NETs are mainly tumors of adults (mean age 52 years), but have also been rarely observed in children.4 There is a male preponderance (73%).4 Whites constituted the highest proportion of patients accounting for 83% of cases.4 In contrast to histologic similar tumors in the lung, there is no established role of smoking.
In one series of thymectomies performed in patients without myasthenia gravis, 12.5% of tumors were found to be epithelial thymic malignancies, one-half of which were carcinoid tumors.5
Thymic neuroendocrine carcinomas exhibit local symptoms (chest pain, cough, dyspnea, or superior vena cava syndrome).1 About 25% of patients have a family history of MEN1.6,7 MEN1-associated thymic NETs/NECs have all been carcinoids and occurred almost only in male adults. No high-grade NETs/NECs have been reported in the setting of MEN1 syndrome. Paraneoplastic manifestations include Cushing syndrome, hypercalcemia (resulting either from tumor production of PTHrP or from primary hyperparathyroidism in MEN1 patients), acromegaly, and inappropriate production of antidiuretic hormone or atrial natriuretic peptide.6,7,8,9,10,11 Paraneoplastic autoimmune disorders, such as the Lambert-Eaton and myasthenic syndromes, and carcinoid syndrome are very rare (<1%).1
Gross Pathology
Well-differentiated (carcinoids) and poorly differentiated thymic neuroendocrine carcinomas are virtually identical macroscopically. The majority of tumors is unencapsulated and can appear either circumscribed or grossly invasive. They are gray-white and firm on cut section, can have a gritty consistency, and usually lack the characteristic lobulated growth pattern of thymomas. Foci of hemorrhage and necrosis are apparent in 70% of cases. Calcifications are frequent.1
Microscopic Pathology
Typical carcinoids (well-differentiated NETs/carcinomas) are devoid of necrotic areas and exhibit a low mitotic rate (<2 mitoses per 10 HPFs). The tumor cells are uniform and polygonal, with relatively small, round nuclei, finely granular chromatin, and pale eosinophilic cytoplasm. Most tumors (>50%) show trabecular and rosetting growth patterns, but a number of other patterns, such as ribbons, festoons, solid nests, glandular structures, and nuclear palisading, are also common. A delicate “endocrine tumor-type” vasculature between the nests and trabeculae is characteristic. Lymphovascular invasion is frequent.
Between 60% and 70% of thymic NETs are atypical carcinoids.2 Atypical carcinoid is defined as a well-differentiated neuroendocrine carcinoma, intermediate grade with (1) mitotic rate of 2 to 10 per 10 HPFs, and/or (2) focal necrosis (Figs. 112.1 and 112.2). Usually, both increased mitotic activity and necrosis are present. Similar to their lung counterparts, the upper limit of mitoses in atypical carcinoid is defined as 10 mitoses per 10 HPFs; tumors exceeding that cutoff are classified as high-grade neuroendocrine carcinomas, subtyped as small cell or large cell neuroendocrine carcinomas.
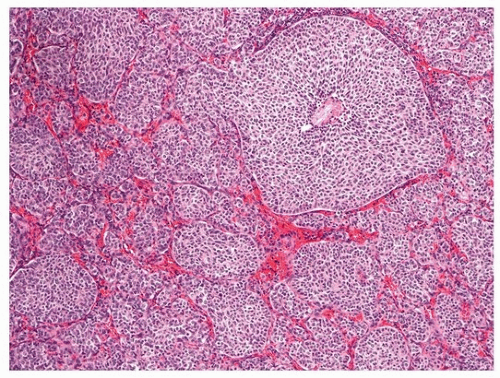 FIGURE 112.1 ▲ Atypical carcinoid (well-differentiated neuroendocrine carcinoma, intermediate grade). Note solid nests and delicate “endocrine tumor-type” vasculature.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|