CHAPTER 31 Thoracoscopic Approach to Spinal Deformities
Introduction
In December 1993, at Children’s Hospital Medical Center in Cincinnati, we began performing VATS for the anterior release of severe spinal deformities in children and adolescents. The benefits of this procedure include minimal invasiveness, better visualization and magnification, diminished postoperative pain and ventilatory compromise, reduced blood loss, decreased hospitalization, reduced health-care costs, improved wound care, and earlier return to prehospital activities with minimal shoulder dysfunction.1
Indications for Children and Adolescents
♦ Rigid idiopathic scoliosis deformities at or above 75 degrees in magnitude with correction to less than 50 degrees seen on side-bending radiographs
♦ Prevention of crankshaft phenomenon in the skeletally immature child who has more than a 50-degree curvature
We have extended our indications to include all the procedures addressing the thoracic spine that were previously approached by thoracotomy.2
Approach to Minimally Invasive Exposure of the Thoracic Spine
Key Points
♦ Working ports should be placed in order to align the instruments fairly straight into the disk spaces.
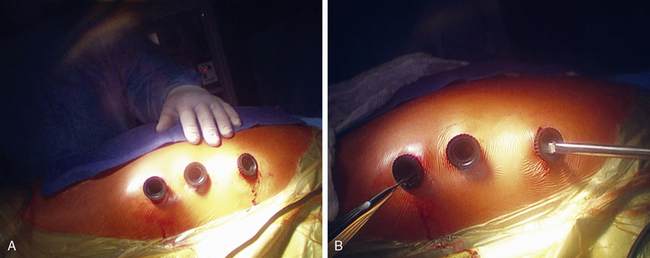
♦ At least three ports are recommended. One port is needed for a pediatric Wolf or Yankauer suction (Scanlon International, St. Paul, Minn). One port is used for the thoracoscope. This leaves one working port. An additional lower port or incision is used for the Endokittner (Ethicon Endosurgery, Cincinnati, Ohio) to depress the diaphragm. By shifting the instruments from port to port, T2 to L1 can be instrumented (Figure 31-1).
♦ The Harmonic scalpel is used to open the parietal pleura and, when indicated, to divide the intercostal vessels.
♦ The endoscopic hardware includes various angled thoracoscopes capable of magnifying up to 15 times, as well as specialized thoracospinal instruments (e.g., rongeurs, curettes, periosteal elevators, electrocautery, Harmonic scalpel, and suction irrigation devices).3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


