Diseases of the thoracic aorta, although relatively uncommon, remain among the most lethal and difficult to treat problems in all of medicine. There are two general categories of aortic disease: aortic dissection and aortic aneurysms.
Acute aortic dissection is the most common aortic emergency, and more than one in four patients die in hospital. Thoracic aortic aneurysms (TAAs) are much less common than abdominal aortic aneurysms (AAAs), but rupture is typically catastrophic and results in sudden death. The overall goal for these entities is aggressive blood pressure management and elective repair, where indicated, to avoid acute events.
ETIOLOGY
TAAs are principally caused by medial degeneration related to atherosclerosis. This accounts for up to three fourths of cases. Additionally, secondary dilatation of aortic dissections accounts for approximately a fifth of cases. The remaining etiologies include inherited abnormality of collagen, spondyloarthropathies, infection, aortitis, and trauma. Two well-described inherited connective tissue disorders that can cause thoracic aortic pathology are Marfan’s syndrome and Ehlers-Danlos’ syndrome. The presence of a bicuspid aortic valve increases the risk of developing an ascending thoracic aneurysm.
Pathophysiology
Aortic aneurysm histopathology, which is more accurately termed medial degeneration, is characterized by disruption and loss of elastic fibers and increased deposition of proteoglycans. Typically, there are areas of loss of smooth muscle cells in the aortic media and the presence of inflammatory cell infiltration in this disease. Aortic pathology associated with myosin heavy chain 11, smooth muscle (MYH11) and actin, alpha 2, and smooth muscle aorta (ACTA2) mutations leading to ascending aortic aneurysms demonstrates a hyperplastic response by smooth muscle cells in the aortic media. Although accumulation of proteoglycans in the aortic media is a consistent finding in TAAs, studies have not determined why this accumulation occurs or whether these are causal in nature.
Clinical Presentation
TAAs are usually asymptomatic but can present as chest, back, abdominal, or flank pain depending on which adjacent structure is compressed, stretched, or eroded into. These include the recurrent laryngeal nerve (hoarseness), bronchus (coughing or stridor), esophagus (dysphagia), or rarely even superior vena cava (upper-extremity edema) or the vertebrae and spinal cord (paralysis). Congestive heart failure due to aortic regurgitation or myocardial ischemia due to coronary compression is common. In many patients, identification of thoracic aneurysm disease occurs only incidentally when they undergo x-rays or tomographic scans for other indications.
Classification
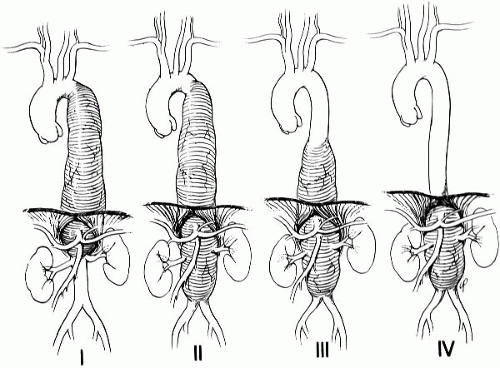
The Crawford classification is important for surgical and endovascular intervention planning. The classification scheme is based on the location and extent of involvement of the descending aorta (Fig. 14.1). This allows patients to be stratified into different risk categories for cardiac, renal, and spinal cord complications. Aneurysms proximal to the left subclavian artery are described on the basis of whether the aortic root or any brachiocephalic branch (arch aneurysms) is involved.
FIGURE 14-1. Crawford classification of thoracoabdominal aneurysms of the descending aorta. Type I involves most of the descending aorta above the renal arteries; type II involves virtually the entire descending aorta; type III involves the distal segment of the thoracic aorta and varying lengths of the abdominal aorta; and type IV involves most or all of the abdominal aorta including the visceral vessels. (From Morrisey NJ, Hamilton IN, Hollier LH. Thoracoabdominal aortic aneurysms. In: Moore WS, ed. Vascular surgery. Philadelphia, PA: WB Saunders, 2002:438.)
Diagnosis
Definitive diagnosis of thoracic aortic disease requires aortic imaging. Selection of the most appropriate imaging study depends on several patientrelated factors (i.e., hemodynamic stability, renal function, and contrast allergy) and institutional capabilities (i.e., availability of individual imaging modalities, technology, and imaging specialist expertise). Consideration should also be given to patients with borderline abnormal renal function (serum creatinine greater than 1.8 to 2.0 mg/dL) by assessing the tradeoffs between the use of iodinated intravenous contrast for computerized tomography (CT) and the risk of contrast-induced nephropathy and between gadolinium agents used with MR and the risk of nephrogenic systemic fibrosis. It is recommended that external aortic diameter be reported for CT- or MR-derived size measurements. This is important because lumen size may not accurately reflect the external aortic diameter in the setting of intraluminal clot, aortic wall inflammation, or dissection.
Chest X-Ray
Chest x-ray is often a part of the evaluation of patients with aortic diseases. However, chest x-ray is inadequately sensitive to definitively exclude the presence of aortic aneurysm or dissection and therefore rarely excludes the disease.
Computerized Tomography
CT has been shown to have 92% accuracy for diagnosing abnormalities of the thoracic aorta, in a series of examinations that included 33 thoracic aneurysms, 3 ruptured TAAs, 6 PAUs, 5 aortic dissections, and 2 pseudoaneurysms. The sequence for CT performed in the potential setting of acute aortic dissection generally would include a noncontrast study to detect subtle changes of intramural hematoma followed by a contrast study to delineate the presence and extent of the dissection flap, identify regions of potential malperfusion, and demonstrate contrast leak indicating rupture. Technical parameters recommended for image reconstruction are slices of 3-mm or less thickness with a reconstruction interval of 50% or less than the slice thickness at 50% or greater overlap, tube rotation of 1 second or less, and 120 to 140 kVp.
Magnetic Resonance Imaging
MR has been shown to be very accurate in the diagnosis of thoracic aortic disease, with sensitivities and specificities that are equivalent to or may exceed those for CT and transesophageal echocardiography (TEE). Black blood imaging, using spin-echo sequences, is used to evaluate aortic anatomy and morphology (such as aortic size and shape) and the aortic wall for hematoma or other causes of thickening, such as vasculitis. Noncontrast white blood imaging is performed using either basic gradient echo sequences or the more advanced balanced steady-state free precession T2-weighted techniques that generate images with subsecond temporal resolution. Signal is generated from blood, making it appear white in the absence of contrast.
Contrast Angiography
Angiography provides accurate information about the site of dissection, branch artery involvement, and communication of the true and false lumens. Additionally, angiographic and catheter-based techniques allow for evaluation and treatment of coronary artery and aortic branch disease, as well as assessment of aortic valve and left ventricular function if indicated. Several disadvantages such as timely availability, exposure to iodinated contrast, and potential false-negative results with a thrombosed false lumen have replaced catheter-based angiography with CT, MR, and TEE as the first-line diagnostic tests to establish the presence of the acute aortic syndrome.
Transesophageal Echocardiography
TEE is safe and can be performed at the bedside, with a low risk of complications (less than 1% overall, less than 0.03% for esophageal perforation). The echocardiographic diagnosis of TAAs is determined on demonstration of aortic enlargement relative to the expected aortic diameter, based on age-adjusted and body size-adjusted nomograms. Overall, the sensitivity for proximal aortic dissection is 88 to 98% with a specificity of 90 to 95%. Advantages of TEE include its portability, rapid imaging time, and lack of intravenous contrast or ionizing radiation. Additionally, dissection-related cardiac complications can be evaluated including aortic regurgitation, proximal coronary artery involvement, and the presence of tamponade physiology. Disadvantages include a potential lack of availability at small centers and during off hours and sedation requirements that may include endotracheal intubation. Furthermore, the accuracy of TEE can be quite operator dependent. The recommendations for aortic imaging techniques to determine the presence and progression of thoracic aortic diseases are outlined in Table 14.1.
MANAGEMENT
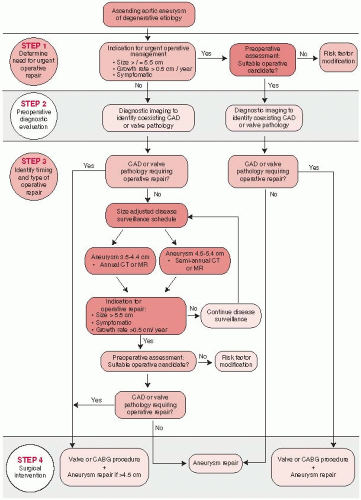
Clinicians should routinely evaluate any patient presenting with complaints that may represent acute thoracic aortic dissection to establish a pretest risk of disease that can then be used to guide diagnostic decisions. This process should include specific questions about medical history, family history, and pain features as well as a focused examination to identify findings that are associated with aortic dissection. Meticulous control of hypertension, lipid profile, smoking cessation, and other atherosclerosis risk-reduction measures should be instituted for patients with small aneurysms not requiring surgery as well as for patients who are not considered to be surgical or stent-graft candidates. The optimal diameter at which a TAA should be repaired is not completely defined. Repair is indicated in asymptomatic patients with degenerative thoracic aneurysm, chronic aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, mycotic aneurysm, or pseudoaneurysm, who are otherwise suitable candidates and for whom the ascending aorta or aortic sinus diameter is 5.5 cm or greater. Patients with Marfan’s syndrome or other genetically mediated disorders (vascular Ehlers-Danlos’ syndrome, Turner’s syndrome, bicuspid aortic valve, or familial TAA and dissection) should undergo elective operation at smaller diameters (4.0 to 5.0 cm depending on the condition; see Chapter 13 also) to avoid acute dissection or rupture. Similarly, patients with a growth rate of more than 0.5 cm/y in an aorta that is less than 5.5 cm in diameter should be considered for operation. Patients undergoing aortic valve repair or replacement and who have an ascending aorta or aortic root of greater than 4.5 cm should also be considered for concomitant repair of the aortic root or replacement of the ascending aorta (Fig. 14.2).
TABLE 14.1 RECOMMENDATIONS FOR AORTIC IMAGING TECHNIQUES TO DETERMINE THE PRESENCE AND PROGRESSION OF THORACIC AORTIC DISEASE
Measurements of aortic diameter should be taken at reproducible anatomic landmarks, perpendicular to the axis of blood flow, and reported in a clear and consistent format.
For measurements taken by computed tomographic imaging or MRI, the external diameter should be measured perpendicular to the axis of blood flow. For aortic root measurements, the widest diameter, typically at the midsinus level, should be used.
For measurements taken by echocardiography, the internal diameter should be measured perpendicular to the axis of blood flow. For aortic root measurements, the widest diameter, typically at the midsinus level, should be used.
Abnormalities of aortic morphology should be recognized and reported separately even when aortic diameters are within normal limits.
The finding of aortic dissection, aneurysm, traumatic injury, and/or aortic rupture should be immediately communicated to the referring physician.
Techniques to minimize episodic and cumulative radiation exposure should be utilized whenever possible.
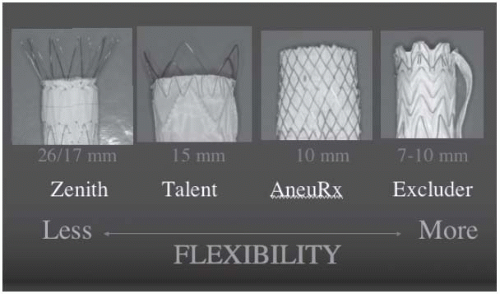
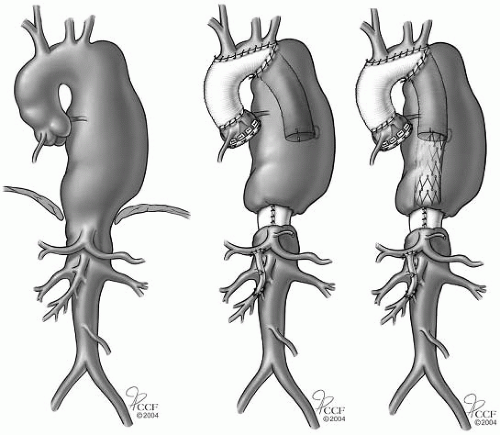
Contemporary management of TAAs has changed substantially with the evolution of endovascular stents (Fig. 14.3). The choice of surgical or endovascular intervention is influenced by aneurysm anatomy, involvement of the arch, and distal extent of the aneurysm. The specifics of operative strategy will vary based on the aneurysm morphology and preference of the surgeon. The most commonly applied surgical techniques include the clamp-and-sew technique. This is supplemented by protective adjuncts, and distal aortic perfusion is often provided as an atriofemoral bypass. An “elephant trunk” procedure has been used to reconstruct the arch and then provide a Dacron graft landing zone for endovascular stent-graft treatment of descending TAAs (Fig. 14.4).
Postoperative paraplegia related to spinal cord ischemia is the most feared nonfatal complication of TAA repair. In an effort to minimize this risk, a variety of adjunctive techniques have been developed. These include cerebrospinal fluid drainage, regional hypothermic protection using ice saline epidural infusion, reimplantation of critical intercostals arteries, evokedpotential monitoring, and distal aortic perfusion via atriofemoral bypass.
FIGURE 14-2. Ascending aortic aneurysm management strategy. (CABG, coronary artery bypass graft surgery; CAD, coronary artery disease; CT, computed tomographic imaging; MR, magnetic resonance imaging.) (Adapted from 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation 2010;121;1544-1579.)
FIGURE 14-3.Types of thoracic stent grafts: proximal fixation segments.
The feasibility of endoluminal stent grafting for TAAs has resulted in renewed evaluation and approach to thoracic aortic treatments. While now firmly established and having three FDA-approved devices, there remains controversy as to optimal indications, technical feasibility, and follow-up. Stent grafts have been applied to a broad range of clinical settings and indications. As a result, the risks of stent grafting the thoracic aorta have been more clearly defined. There is, however, a lack of long-term follow-up data and ongoing controversy as to a complete understanding of the risk-benefit ratio of stent grafting versus either medical management or open surgical repair.
Recently reported literature has reported a wide variation in operative mortality between 2 and 26%. This variation has largely been related to the urgency of the procedure, the extent of comorbid disease, and the experience of the operator. Analysis of midterm results demonstrates a 3- to 8-year survival of 25 to 90% over a broad range of clinical indications. Despite low operative mortality, thoracic stent grafting has been associated with a variety of late complications. These complications include endoleaks, graft migration, stent fractures, and aneurysm-related deaths. The late complications are reported much more commonly than what has been reported with open surgical repair.
The indication for stent grafting of descending TAAs needs to be based on the predictive operative risk that is lower than the risk of either conventional open repair or medical management. Consideration of a patient’s age, comorbidity, life expectancy, and quality of life is significant. Aneurysm morphology and adequacy for stent grafting along with operator experience are also relevant considerations. It is also important to remember that postprocedure surveillance involves routine CT scans, and aortic reintervention is commonly required.
FIGURE 14-4. Elephant trunk procedure. Left: Preoperative disease. Middle: Stage I with replacement of the ascending aorta and arch with a Dacron graft with the distal graft sutured circumferentially to the aorta distal to the left subclavian artery and the free end of the graft (“elephant trunk”) within the descending aneurysm. Right: Completion of the procedure using an endovascular stent graft attached proximally to the “elephant trunk” and the distal end secured to a Dacron graft cuff. (Adapted from 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation 2010;121;1544-1579.) (See color insert.)
The Gore TAG phase II study provides the best currently available comparison of open versus surgical treatment of descending TAAs. In this nonrandomized trial, TAG devices were placed in 137 patients, and compared to an open surgical control of 94 patients, 44 were concurrent and 50 historical. Perioperative mortality was 2.1% with endografting and 11.7% with open surgery. A 30-day analysis of complications demonstrated a significantly lower incidence of spinal cord ischemia, 3% versus 14%; reduced respiratoryfailure, 4% versus 20%; and reduction of renal failure, 1% versus 13%. Peripheral vascular complications were higher in the endograft cohort, that is, 14% versus 4%. Follow-up at 1 and 2 years demonstrated an endoleak rate of 6 and 9%, respectively, and reintervention in three endograft patients at 2 years. No reintervention was required in the surgical group. No difference in overall mortality was observed at 2 years by Kaplan-Meier analysis. Additional data have been forthcoming from a number of industry-sponsored trials. The VALOR trial using Medtronics Talent device completed enrollment in 2005. The PIVITOL group consisted of patients with degenerative thoracic aneurysms who were considered to be at low-to-moderate risk for surgical repair. Thirty-day mortality was 2.1% with a paraplegia rate of 1.5% and a stroke rate of 3.6%. All-cause mortality was reported at 1 year of 16.1 % with aneurysm-related death of 3.1 %. The STARZ trial was sponsored by Cook and used the Zenith TX2 endograft device. Enrollment was completed in 2006. Thirty-day mortality was 1.9% compared to 5.7% in the surgical control. Major preoperative events were also lower in the endograft group, 2.5% versus 7.1%. The incidence of paraplegia was 1.3% in the stent-graft group compared to 5.7% in the control group.
Only gold members can continue reading. Log In or Register to continue