Fig. 12.1
Apical 4-chamber view demonstrating the dilated right atrium and right ventricle. RA right atrium, RV right ventricle, LA left atrium, LV left ventricle
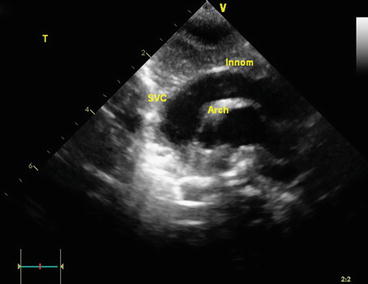
Fig. 12.2
Suprasternal long-axis view showing dilated superior vena cava and innominate vein resulting from increased venous return. Also seen is the transverse arch inferior to innominate vein. SVC superior vena cava, Innom innominate vein
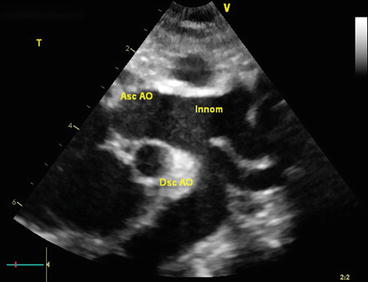
Fig. 12.3
Sagittal image from the suprasternal notch of the aortic arch. There is a dilated proximal innominate artery and the left common carotid. Note narrowing of the transverse arch and aortic isthmus. Asc AO ascending aorta; Innom, brachocephalic trunk (also giving rise to left common carotid artery in this patient); Dsc AO descending aorta
Discussion
Arteriovenous malformations are high-flow communications due to absence of a developed capillary bed. They can occur in various organs, and presenting features can vary greatly depending on patient age, lesion size and location. Vein of Galen malformations are the most common form of symptomatic cerebrovascular malformation in neonates and infants. They account for less than 1–2 % of all intracranial vascular malformations but are the cause of 30 % of cerebral vascular malformations presenting in the pediatric age group. It is also the most common antenatally diagnosed intracranial vascular malformation. The malformation is due to a cerebral arteriovenous fistula of the median prosencephalic vein (MPV) (a precursor of the vein of Galen) occurring at 6–11 weeks of gestation, which fails to regress and becomes aneurysmal.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


