Fig. 8.1
Subcostal 5-chamber view showing a doming aortic valve (red arrow) and moderate pericardial effusion (blue arrow)
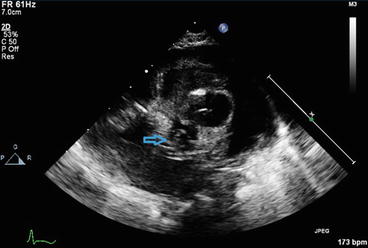
Fig. 8.2
Parasternal short-axis view of the aortic valve showing a unicuspid aortic valve (blue arrow)
Fig. 8.3
(a) Doppler evaluation of aortic valve from suprasternal angle at presentation showing a peak velocity of 2.47 m/s (peak gradient 24 mmHg, mean gradient 9 mmHg). (b) Post balloon aortic valvotomy continuous wave Doppler evaluation from the suprasternal angle, showing peak velocity of 4.67 m/s. The gradient has “increased” in the setting of improved cardiac output
It is easy to underestimate valve gradients in the setting of reduced ventricular function. The presentation of a collapsed neonate, an anatomically abnormal aortic valve on 2D imaging, and poor left ventricular function support the diagnosis of critical aortic stenosis. The pericardial effusion was the result of poor left ventricular function and not the cause of heart failure.
The patient underwent balloon aortic valvoplasty and pericardiocentesis during the same procedure. Valvoplasty achieved a good angiographic result, with substantial improvement in aortic valve opening and forward flow into the ascending aorta. There was significant clinical improvement, and the infant was extubated within a few hours. The post-procedure echocardiogram showed an improvement in LV contractility, but the peak transvalvar gradient was now 88 mm Hg (see Fig. 8.3b). There was mild aortic regurgitation. He remained well, and underwent elective surgical valvotomy at 3 months of age, with an excellent result.
Discussion
Collapse in the neonatal period may have a number of causes, but cardiac ones are amongst the most common. Critical obstruction to the left heart, such as critical aortic stenosis, hypoplastic left heart syndrome, coarctation of the aorta and interrupted aortic arch, present with acute deterioration at the time of ductal closure. Antenatal diagnosis of congenital heart disease allows appropriate management strategies to be put in place to ensure that the baby stays well from birth and acute collapse is pre-empted. Other cardiac causes of neonatal collapse include myocarditis, tachyarrhythmias and complete heart block.
Echocardiography is the cornerstone of diagnosis of congenital heart disease. In patients with left-sided obstructive lesions, echocardiography gives information regarding structure, function and haemodynamics, and will enable the cardiologist to direct management accordingly. Understanding the limitations of echocardiography is very important for the practitioner in the process of reaching a diagnosis.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


