The Role of Fractional Flow Reserve in the Catheterization Laboratory
The Role of Fractional Flow Reserve in the Catheterization Laboratory
Nico H.J. Pijls
William F. Fearon
The inability of coronary angiography to consistently reflect the severity of coronary stenoses is well documented. Despite the fact that inducible ischemia determines the prognosis of our patients, the vast majority of clinical decisions continue to be based on this lumenogram. Several approaches have been developed to determine more accurately the significance of stenoses detected at angiography. Of these, coronary pressure-derived fractional flow reserve (FFR) is the most useful and practically applicable index for clinical decision making.
Coronary pressure measurement is an accurate, easily applicable, and well-validated technique to assess the hemodynamic significance of coronary artery disease, to support decision making with respect to revascularization, and to evaluate the results of percutaneous coronary intervention (PCI).
From a historical perspective, Grüntzig already had the perception that coronary pressure measurement contained useful information to evaluate the functional significance of a stenosis (1).
However, pressure measurement in those days was hampered by three shortcomings: (a) no device existed to measure coronary pressure reliably. Early operators used hypodermic tubes or balloon catheters, which resulted in often severe and unpredictable overestimation of pressure gradients; (b) the importance of maximum hyperemia was not recognized; and (c) the importance of the distal hyperemic perfusion pressure, and not the gradient alone, in determining the extent of ischemia and the patient’s limitations was insufficiently appreciated.
These issues are adequately addressed today. First, reliable 0.014-inch guidewires are available to measure coronary pressure. The influence of these guidewires on the pressure gradient and the distal coronary pressure is negligible, except in the setting of a very tight stenosis, in which case the hemodynamic significance of the stenosis is beyond discussion (2,3).
Second, it is well recognized that measurements should be performed at maximum hyperemia. Most patients with coronary artery disease do not have angina at rest. But with exercise and the increase in myocardial oxygen demand, blood flow must increase to meet this demand; if this cannot occur, for example because of a coronary stenosis, angina will develop. Therefore, maximum achievable blood flow, rather than resting flow, is necessary to accurately characterize the hemodynamic significance of a coronary artery stenosis.
Third, it should be realized that it is not the stenosis gradient itself but the resulting distal perfusion pressure that determines the hemodynamic significance of a stenosis. To know the significance of the stenosis for a patient, it is not relevant to know the stenosis dynamics or pressure flow relationship across the stenosis, but it is sufficient to know the common effect of all those variables on the distal coronary perfusion pressure at hyperemia. These considerations are reflected by the concept of FFR (5,6).
Figure 6.1.
Upper panel
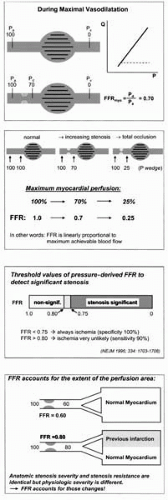
Schematic illustration of the principle of FFR. During maximum vasodilation, myocardial perfusion pressure is directly proportional to maximum myocardial blood flow. In a normal coronary artery, hyperemic distal perfusion pressure equals aortic pressure and, therefore, in this example, myocardial perfusion pressure equals 100 mm Hg.
Suppose now that a coronary stenosis exists in the supplying conduit artery and that, as a result of this stenosis, hyperemic distal coronary pressure has decreased to 70 mm Hg. In that case, myocardial perfusion pressure has decreased to 70 mm Hg as well. Because of the proportionality between perfusion pressure and myocardial blood flow, maximum myocardial perfusion in the presence of the stenosis is only 70% of the hypothetical value it should be if the supplying artery were completely normal.
The fraction of normal maximum blood flow maintained despite the presence of the stenosis is 0.70 or 70%. This fraction is called myocardial fractional flow reserve (FFR or FFRmyo) and equals distal perfusion pressure in the stenotic artery measured during maximum myocardial vasodilation, divided by aortic pressure. Thus, the ratio of maximum flows can be expressed as a ratio of perfusion pressures.
Second panel
One of the unique features of FFR is that it is related in a linear way to the decrease of maximum flow of the myocardium. With increasing stenosis severity, decrease of maximal achievable coronary blood flow is directly indicated by the decrease of FFR. At total occlusion, myocardial flow is reduced to collateral flow, which is still expressed by FFR as a ratio to normal maximum flow.
Third panel
It has been well demonstrated that fractional flow reserve separates lesions of hemodynamic importance (i.e., associated with inducible ischemia) from lesions without ischemic potential. Only a very small gray zone exists between 0.75 and 0.80. Below 0.75, intervention is always justified. Above 0.80, it is extremely unlikely that the respective lesion causes ischemia, and revascularization is generally not necessary or beneficial.
Lower panel
FFR also matches stenosis severity to the extent of the perfusion area. This is also a unique feature of fractional flow reserve. In two different patients, with a similar stenosis severity, similar anatomy, and similar stenosis resistance, but a different extent of myocardium to be supplied (as is the case, for example, after previous MI), the difference in functional severity of the lesions is accounted for by FFR. Because of the higher vasodilatory capacitance of the larger perfusion territory, FFR is lower.
FRACTIONAL FLOW RESERVE
Fractional flow reserve (FFR) is defined as the maximum achievable myocardial blood flow in the presence of a coronary artery stenosis, in relation to the maximum blood flow in the hypothetical case that the artery is completely normal. Under maximum arterial vasodilation, the resistance of the myocardium is minimal and constant (7, 8, 9) and thus blood flow to the myocardium is proportional to the “driving pressure” or myocardial perfusion pressure (Fig. 6.1, upper panel). In normal coronary arteries, no pressure gradient exists along the coronary artery itself, not even at maximum hyperemia (6,10). Therefore, in a normal epicardial coronary artery, the myocardial perfusion pressure equals aortic pressure minus central venous pressure, the latter being generally close to zero.
In the case of a stenosis in the coronary artery, distal coronary pressure will decrease, and it is this distal pressure during hyperemia (minus central venous pressure) which is the actual perfusion pressure for the myocardial territory supplied by the stenotic coronary artery. Because of the constancy of the resistance of the myocardial vascular bed at hyperemia (and the linear proportionality between perfusion pressure and myocardial flow), maximum blood flow in the stenotic situation can be expressed as a ratio to normal maximal blood flow by taking the ratio of the respective perfusion pressures—that is, distal coronary pressure at hyperemia divided by aortic pressure.
Therefore, this ratio of maximum flows can be calculated easily by a ratio of pressures and expressed as:
where Pa′ Pd′ and Pv represent aortic, distal coronary, and central venous pressure, respectively.
In fact, FFR represents the very fraction of normal maximum myocardial blood flow still achievable despite the presence of the stenosis (4,6).
If FFR equals 0.6, this simply means that, as a result of the stenosis, maximum myocardial flow is only 60% of what it should be in the normal case (Fig. 6.1, second panel). And if this value increases to 0.9 after PCI, it means that maximum flow (and thus, oxygen supply to the myocardium) has increased by 50%.
The concept and assumptions of FFR have been well validated both in experimental and clinical studies (3, 4, 5, 6, 7, 8, 9, 10, 11, 12).
FEATURES OF FRACTIONAL FLOW RESERVE
A number of features of FFR make it a valuable index for everyday use in the catheterization laboratory, both at diagnostic and interventional procedures.
These features are listed in Table 6.1 and are discussed briefly in upcoming sections of this chapter.
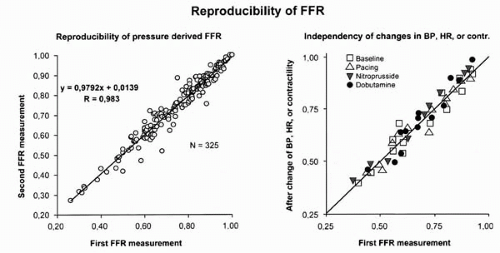
Unlike most other indexes, FFR has a uniform normal value of 1.0 for every patient and every coronary artery (6,10). In addition, it does not vary with changes in heart rate, blood pressure, or contractility (13, 14, 15) (Fig. 6.2). Therefore, unlike classical coronary flow reserve, the interpretation of a value of FFR is not affected by interindividual variability.
FFR is an index of myocardial blood flow, not only coronary blood flow, and takes into account the collateral flow (4, 5, 6,8). Therefore, from the point of view of the patient, it is a better descriptor of the severity of coronary artery disease than those indexes that only take into account the coronary artery blood flow. Importantly, FFR specifically indicates the effect of the epicardial abnormalities on myocardial blood flow. In contrast to FFR, it is not confounded by microvascular abnormalities (7,8). It is even possible to calculate separately the contribution of coronary arterial and collateral blood flow to myocardial blood flow, as discussed in the upcoming section on FFR used to assess the result of coronary intervention and more extensively in the literature (5,6,16).
A circumscript threshold of ischemia exists for FFR that allows the discrimination of functionally significant stenoses (Fig. 6.1, third panel). This sharp threshold of 0.75 to 0.80 has been confirmed prospectively in many studies and under many angiographic conditions (3,6,17, 18, 19). FFR is the only physiologic index that has been validated against a true gold standard of inducible ischemia (4). A FFR below 0.75 is almost always associated with inducible ischemia (specificity of the index close to 100%), whereas a value above 0.80 indicates the absence of inducible ischemia in the majority of patients (sensitivity 90%).
TABLE 6.1. FEATURES OF FRACTIONAL FLOW RESERVE
Uniform normal value of 1.0 for every artery and every patient
Linear relation to maximum blood flow
Not influenced by changes in heart rate, blood pressure, or contractility
Specific index of epicardial stenosis
FFR accounts for total myocardial blood flow, including collaterals
Sharp threshold of ischemia (0.75-0.80)
Easy to measure and extremely reproducible
FFR matches the stenosis severity to the extent of the perfusion area
Figure 6.2.(Left panel) Reproducibility of FFR in a multicenter study in 325 patients, in whom FFR was measured twice with an interval of 10 minutes. (Right panel) Reproducibility of FFR during hemodynamic interventions such as changes in heart rate (triangles), blood pressure (inversed triangles), and contractility (dots).
Despite variations in heart rate of 40%, variation in blood pressure of 35%, and variation of contractility of 50%, FFR was not affected by these changes. (Reprinted with permission from Circulation 2001;103:2928-2934 and Circulation 1996;94:1842-1849.)
Therefore, because the gray zone is so narrow, FFR is a suitable index to discriminate if a particular stenosis or plaque is associated with inducible ischemia or not, with major implications for decision making (3).
From the practical point of view, FFR is easy to measure, having a success rate of almost 100%; the measurements can be done quickly within minutes; and the index is extremely reproducible, as demonstrated in several large studies (20, 21, 22) (Fig. 6.2). Variability between paired measurements is typically in the range of 0% to 3%. FFR can be applied in many clinical situations, as described in upcoming sections. In contrast to indexes focusing on the coronary artery, FFR also can be used after previous myocardial infarction (MI) because it matches the stenosis severity to the extent of the perfusion area (17).
Finally, coronary pressure measurement has an unequaled spatial resolution to discriminate different abnormalities or diffuse disease along the course of the coronary artery, as explained in the section on pressure pullback recording. In this respect, coronary pressure measurement is unique and more precise than any other invasive or noninvasive technique (23, 24, 25).
Finally, FFR has a direct clinical and pathophysiologic equivalent: a value of FFR of 0.60 measured in a particular coronary artery indicates that the artery is diseased to such an extent that the maximum amount of blood flowing to the myocardium subtended by that artery has decreased to only 60% of what it should be in a normal case. If this value improves after PCI to 0.90, it indicates that the maximum blood flow to the myocardium has increased by 50%. An FFR of 0.90 means twice as much blood flow to the myocardium during hyperemia than an FFR of 0.45. So, FFR is linearly related to maximum flow (Fig. 6.1, second panel). The range of FFR is from approximately 0.25 (total occlusions, collateral flow) to 1.0 (completely normal artery) (6,10,26).
PRACTICE OF CORONARY PRESSURE MEASUREMENT
Equipment Needed to Measure Coronary Pressure
Presently, two Food and Drug Administration (FDA)-approved pressure wires are available for measuring FFR (Pressure Wire, Radi Medical System, Reading, Massachusetts; and Smart Wire, Vulcano Therapeutics Inc, Rancho Cordova, California). Both wires can be used as percutaneous transluminal coronary angioplasty (PTCA) guidewires with mechanical properties close to normal guidewires.
A pressure sensor is present 3 cm from the tip of both wires, at the junction of the radio-opaque and radiolucent portion. Therefore, the pressure sensor can be moved across a coronary artery stenosis and back again (showing the pressure drop) without the necessity of crossing the stenosis with the tip time and again (27,28).
An interface is available to record and analyze the data or to transfer the data to the regular catheterization laboratory monitoring system.
Both wires can be connected and disconnected by an interface cable. When connected, pressures are measured; when disconnected, a balloon catheter, stent, or other interventional equipment can be advanced. It is generally recommended to use 6 Fr guiding catheters, but all other guiding or diagnostic catheters can be used as well.
Suggested Protocol for Coronary Pressure Measurement
When measuring FFR, heparin and nitroglycerin are administered in the usual fashion, and the pressure wire is advanced until the sensor is at the tip of the guiding catheter. At this point, it is verified that equal pressures are recorded from the wire and the catheter. The wire is then advanced down the coronary artery and across the stenosis, or to the distal part of the coronary artery in case of multiple abnormalities or diffuse disease (Fig. 6.3).
Next, a hyperemic stimulus is administered (Table 6.2), blood flow is maximized, and distal pressure minimized. At that moment, FFR is calculated as the ratio between the distal coronary pressure (measured by the pressure wire) and aortic pressure (measured by the guiding catheter).
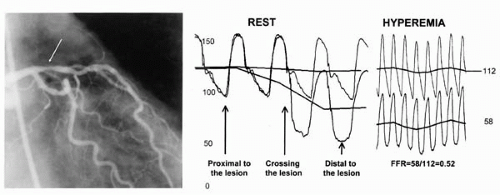
Figure 6.3. Measurement of FFR in a 77-year-old patient with an intermediate lesion in the proximal left anterior ascending artery. Phasic and mean pressure signals are displayed as recorded by the guiding catheters and the sensor-tipped pressure wire.
On the left hand of the pressure tracing, the pressure sensor is proximal to the stenosis, and two exactly identical pressures are found. It can be observed how distal pressure decreases as soon as the pressure sensor crosses the stenosis.
To unmask the full ischemic potential of that stenosis, maximum hyperemia is induced. During maximum hyperemia (right-hand side of the pressure tracing), hyperemic distal pressure decreases to 58 mm Hg, resulting in an FFR of 0.52. Thus, due to the stenosis in the proximal LAD artery, maximum blood flow to the myocardium of the anterior wall of this patient is decreased to only 52% of normal. Not only the severity of the stenosis, but also its exact location can be nicely illustrated in this way.
TABLE 6.2. MAXIMUM HYPEREMIC STIMULI
Papaverine i.c.
(10 mg, RCA, 15-20 mg LCA)
Adenosine or ATP i.c.
(30 μg RCA, 40-80 μg LCA)
Adenosine or ATP i.v.
(140 μg/kg/min in central vein)
NOTE:
Maximum hyperemia is paramount to determine FFR
Sometimes, incremental doses of i.c. adenosine or ATP might be necessary
Intravenous adenosine or ATP preferably by femoral vein (most reliable and quick) or large antecubital vein (longer infusion necessary)
Fluctuations in hyperemic level might be related to breathing. FFR always taken as the lowest value of Pd/Pa (peak hyperemia)
To study the distribution of abnormalities along a diseased coronary artery, the wire can be pulled back slowly during hyperemia, nicely indicating at which particular locations hemodynamically significant abnormalities are present (Fig. 6.4). If PCI of one or more lesions is necessary, the wire may be disconnected, the intervention performed, and the pressure measured again by reconnecting the wire. In this way, both an angiographic and a hemodynamic assessment of the intervention can be made (Fig. 6.4). During balloon occlusion, coronary wedge pressure can be measured and used to quantify recruitable collateral flow (16).
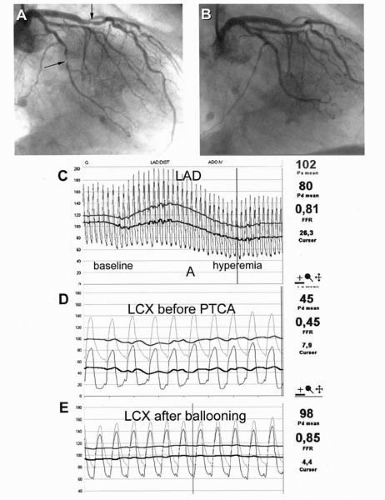
Figure 6.4. Complex multivessel disease in a 60-year-old man who underwent a stent implantation in the mid-right coronary artery 1 year earlier and who presented with recurrent typical angina and a positive nuclear scan in the inferior wall. The patient was initially referred for bypass surgery but after the pressure measurements, he was treated well by balloon angioplasty of the small circumflex branch and two stents in the right coronary artery.
In the left coronary artery, a 50% stenosis exists in the mid LAD with an FFR of 0.81 (panels A and C). Therefore, it is unlikely that the LAD contributes to inducible ischemia.
Furthermore, a focal stenosis is present in the small circumflex branch, which is significant according to an FFR of 0.45 (panels A and D). After plain balloon angioplasty of the LCX-stenosis, a satisfying angiographic result occurs, and FFR has almost doubled to 0.85 (panels B and E).
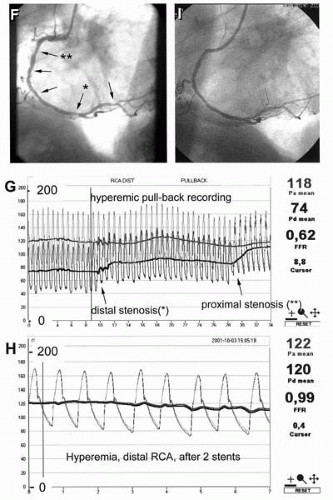
The right coronary artery shows diffuse disease with at least 5 stenoses of intermediate severity (panel F).
FFR of the distal myocardium supplied by the RCA equals 0.62 (panel G). The pressure pullback curve at hyperemia shows that two of these multiple plaques are hemodynamically significant, indicated by the asterisks.
The other plaques do not have hemodynamic significance. Consequently, two stents were placed at the locations indicated by the asterisks, whereas a reasonable angiogram and an excellent functional result was obtained with normalization of FFR (panels H and I).
The most powerful application of coronary pressure measurement in the catheterization laboratory, essential for strategic decision making, is the pressure pullback recording, as demonstrated in the right coronary artery of this patient. By such pullback recording, detailed spatial information can be obtained about all the abnormalities along a diseased coronary artery.
Figure 6.4. (continued)
If multiple stenoses are present, the pullback recording can be repeated after any step to monitor the progress (12,24,25,28). At the end of the procedure, when the sensor is back at the tip of the guiding catheter, equal pressures should be recorded by the guiding catheter and the pressure wire, ensuring that no pressure drift has occurred.
These maneuvers can be performed with little prolongation of the procedure. The technique is easy for an interventional cardiologist, and the risk does not exceed that of a normal procedure. The learning curve is short (29).
Some potential practical pitfalls exist that easily can be avoided and will be discussed later.
IMPORTANCE OF MAXIMUM HYPEREMIA
For the evaluation of the hemodynamic significance of a coronary stenosis, maximum hyperemia is of paramount importance. Only under hyperemic conditions is distal myocardial resistance minimal and constant and can FFR be calculated. By definition, FFR implies maximum hyperemia. Generally, one can talk about the Pd/Pa ratio, but one should realize that this ratio has little clinical value if not determined at maximum hyperemia. Furthermore, by definition, only one value of FFR exists per vessel. This value is the ratio of Pd/Pa at maximum hyperemia, with the pressure sensor placed in the most distal part of the vessel. In this manner, the contribution of multiple lesions or diffuse disease can be quantified in its entirety. By slowly pulling back the pressure sensor during maximum hyperemia, the ratio of Pd/Pa will approach 1, and the area of the vessel where the greatest pressure decrement occurs can be identified.
A number of hyperemic stimuli are used in clinical practice; each has advantages and disadvantages (Table 6.3). Intracoronary adenosine, intravenous adenosine, and intracoronary papaverine are the most common agents used and are reviewed in upcoming sections (15,25).
Intracoronary adenosine creates a very short-lasting maximum hyperemia (approximately 5 seconds) in the majority of patients, if the dosage is high enough. In contrast to some earlier studies, the recommended dosage at present is at least 40 μg for the left coronary artery and 30 μg for the right coronary artery (15,25). If any doubt is present about maximum hyperemia, higher dosages should be used. Intracoronary adenosine is very safe, with clinically insignificant transient bradycardia as its only side effect. Due to its short action, it is suitable to analyze the FFR in the setting of a single coronary stenosis, but it is less suitable in the presence of multiple abnormalities or diffuse disease because its action is too short to allow a pressure pullback recording at hyperemia. When dealing with an ostial right coronary lesion or left main lesion, accurately measuring FFR using intracoronary adenosine is challenging, because the guide catheter must be removed from the coronary ostium immediately after administering the adenosine. Intravenous adenosine is a better option in such cases.
Intravenous adenosine, administered by preference in a central vein at a dosage of 140 μg/kg/min, creates maximum steady-state hyperemia in almost all patients (25,30,31). During administration, most patients experience chest discomfort or dyspnealike complaints, which often resemble angina pectoris. It should be emphasized that this is not an expression of ischemia and that this phenomenon is completely harmless. This reaction is due to the stimulation of free nerve fibers in the heart by the adenosine (which is also the intrinsic transmitter of angina pectoris). If the patient is well informed beforehand, this is never a reason to stop the infusion. This discomfort should not be confused with very rare bronchospasm that can occur in some patients with severe obstructive pulmonary disease. Although bronchospasm is rare, severe asthma is considered a contraindication for intravenous adenosine administration.
Moreover, during the intravenous administration of adenosine, the patient should be instructed to breathe normally and avoid Valsalva maneuvers because this can interrupt the continuous administration of adenosine to the heart and may lead to fluctuation of achieved coronary blood flow, distal pressure, and measured FFR. If respiratory variations are present, FFR always should be taken as the lowest value of Pd/Pa during the respiratory cycles.
Intravenous adenosine enables reliable and steady-state maximum hyperemia for making a pressure pullback recording. Therefore, especially in the setting of multiple abnormalities along a coronary artery, intravenous adenosine is the most reliable way to analyze the functional significance of disease along every portion of the artery. Intracoronary or intravenous ATP, which is not available in the United States, is another hyperemia agent used in a similar fashion to adenosine.
TABLE 6.3. FFR: THE PRESSURE PULLBACK RECORDING
Place sensor in distal coronary artery.
Induce sustained maximum hyperemia by i.v. adenosine, or i.c. papaverine.
Pull back the sensor slowly under fluoroscopy (can be done manually).
If a focal pressure drop is present, it can be confirmed by moving the sensor across the stenosis and back again. The individual contribution of every segment and spot to the extent of disease can be studied in this way and the correct position to place the stent(s) can be unequivocally determined.
In case of multiple spots under consideration to be stented, the pullback curve can be repeated after every step.
In case of a gradual decline of pressure along the artery, without focal pressure drops, stenting makes no sense and medical treatment is indicated.
Coronary pressure is unique in this respect, and such detailed spatial information cannot be obtained by any other invasive or noninvasive technique.
Only gold members can continue reading. Log In or Register to continue