Lifestyle and nutrition have been increasingly recognized as central factors influencing vascular nitric oxide (NO) production and erectile function. This review underscores the importance of NO as the principal mediator influencing cardiovascular health and erectile function. Erectile dysfunction (ED) is associated with smoking, excessive alcohol intake, physical inactivity, abdominal obesity, diabetes, hypertension, and decreased antioxidant defenses, all of which reduce NO production. Better lifestyle choices; physical exercise; improved nutrition and weight control; adequate intake of or supplementation with omega-3 fatty acids, antioxidants, calcium, and folic acid; and replacement of any testosterone deficiency will all improve vascular and erectile function and the response to phosphodiesterase-5 inhibitors, which also increase vascular NO production. More frequent penile-specific exercise improves local endothelial NO production. Excessive intake of vitamin E, calcium, l -arginine, or l -citrulline may impart significant cardiovascular risks. Interventions discussed also lower blood pressure or prevent hypertension. Certain angiotensin II receptor blockers improve erectile function and reduce oxidative stress. In men aged <60 years and in men with diabetes or hypertension, erectile dysfunction can be a critical warning sign for existing or impending cardiovascular disease and risk for death. The antiarrhythmic effect of omega-3 fatty acids may be particularly crucial for these men at greatest risk for sudden death. In conclusion, by better understanding the complex factors influencing erectile and overall vascular health, physicians can help their patients prevent vascular disease and improve erectile function, which provides more immediate motivation for men to improve their lifestyle habits and cardiovascular health.
The identification of nitric oxide (NO) as the long-sought vascular endothelium–derived relaxing factor resulted in the awarding of a Nobel Prize and a continuing explosion of research in vascular pathophysiology and treatment. The enzyme responsible for NO production, NO synthase (NOS), exists as an endothelial enzyme, endothelial NOS (eNOS), and as a neuronal enzyme, neuronal NOS (nNOS), allowing NO to function as an autocrine and paracrine signal and as a neurotransmitter. The discovery of NO led to experiments by 1 of us (L.J.I.) that defined the role of NO in relaxation of smooth muscle of human corpus cavernosum tissue caused by electrical stimulation of nonadrenergic, noncholinergic nerves. Because NO was shown to cause penile smooth muscle relaxation by stimulating cyclic guanosine monophosphate, and the effect was enhanced by a phosphodiesterase-5 (PDE-5) inhibitor of cyclic guanosine monophosphate degradation, this work led to the development of sildenafil, tadalafil, and vardenafil as highly effective treatments for men with erectile dysfunction (ED). PDE-5 inhibitors, however, primarily shore up cyclic guanosine monophosphate levels rather than correcting the inadequate NO production causing poor erectile and vascular function. NO supports vascular health by inhibiting platelet aggregation and the adhesion of platelets and inflammatory cells to the endothelium, opposing vascular smooth muscle proliferation, maintaining low vascular muscle tone, and preventing atherosclerosis by acting as an anti-inflammatory agent and by reducing oxidative stress and endothelial cell senescence.
The Link Between Erectile Dysfunction and Vascular Diseases
ED is defined as the persistent inability (by standardized questionnaires) to obtain and/or maintain penile erection sufficient for satisfactory sexual performance. Coronary risk factors in midlife predict later development of ED. In men with ED, penile systolic velocity is correlated with ischemic heart disease. Because men with ED develop coronary artery calcification at a younger age than controls, ED has been called “penile angina.” In that study, a significant decrease of systemic vascular NO was documented in the patients with ED. The mean ± SE flow-mediated dilation was 2.4 ± 0.21% in the men with ED, compared to 3.9 ± 0.26% in the men without ED (p <0.001). Studies have also found strong correlations of ED with the metabolic syndrome, increased C-reactive protein, and an increased ratio of total cholesterol to high-density lipoprotein. Two thirds of men with angiographically proved coronary artery disease (CAD) had symptoms of ED an average of 39 months earlier.
Although the incidence of ED in men aged 40 to 70 years was reported to be 52%, when men without indications of CAD were screened, the prevalence of ED was only 2% for men aged 40 to 49 years, increasing to only 39% for men aged ≥70 years. New ED in men aged 40 to 49 years was associated with a 50-fold increase in the incidence of CAD (including sudden death) over the following 10 years, whereas the predictive value decreased with increasing age as expected (5.4-fold for ages 50 to 59 years, 2.2-fold for ages 60 to 69 years, and 1.3-fold for age ≥70 years).
Erectile function is adversely influenced by poor lifestyle choices that can lead to more widespread vascular disease, disability, and even death. We discuss the interventions available to improve erectile and overall vascular health.
Exercise
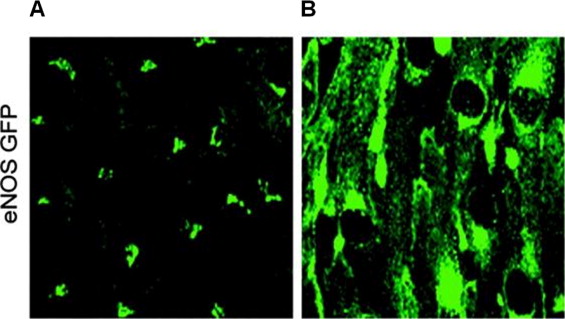
An integral factor stimulating NO release from the endothelium is the mechanical shear force of blood flow ( Figure 1 ). Shear stress induces an immediate release of NO due to an influx of calcium into the endothelial cell and phosphorylation of eNOS and a sustained release by increasing eNOS messenger ribonucleic acid transcription and stability. In men with CAD, daily exercise doubled endothelium-dependent vasodilation and eNOS and tripled eNOS phosphorylation. Whereas acute exercise increases NO release for 48 hours, daily exercise induces fourfold higher levels of NO production for 1 week. Exercise also stimulates NO production by increasing the sensitivity of endothelial NO release to insulin. In that study, insulin-induced vasorelaxation increased by 2/3 after 12 weeks of exercise training (p <0.01), and the effect of insulin, with or without exercise, was abolished by an inhibitor of NO production. Sedentary men are 2 to 3 times more likely to have ED, and ED is associated with hours of television viewing as an indicator of inactivity. Moderate physical activity reduces the risk for ED by 2/3, and in men with high physical activity, the ED risk is reduced by >80%. In obese men, physical activity is strongly associated with improved erectile function.
Exercise
An integral factor stimulating NO release from the endothelium is the mechanical shear force of blood flow ( Figure 1 ). Shear stress induces an immediate release of NO due to an influx of calcium into the endothelial cell and phosphorylation of eNOS and a sustained release by increasing eNOS messenger ribonucleic acid transcription and stability. In men with CAD, daily exercise doubled endothelium-dependent vasodilation and eNOS and tripled eNOS phosphorylation. Whereas acute exercise increases NO release for 48 hours, daily exercise induces fourfold higher levels of NO production for 1 week. Exercise also stimulates NO production by increasing the sensitivity of endothelial NO release to insulin. In that study, insulin-induced vasorelaxation increased by 2/3 after 12 weeks of exercise training (p <0.01), and the effect of insulin, with or without exercise, was abolished by an inhibitor of NO production. Sedentary men are 2 to 3 times more likely to have ED, and ED is associated with hours of television viewing as an indicator of inactivity. Moderate physical activity reduces the risk for ED by 2/3, and in men with high physical activity, the ED risk is reduced by >80%. In obese men, physical activity is strongly associated with improved erectile function.
Obesity, Diabetes, Insulin, and Insulin Resistance
Obesity is a state of chronic inflammation, oxidative stress, and insulin resistance. Obesity is strongly associated with ED, although its major impact is through vascular risk factors associated with obesity. In diabetic men, the prevalence of ED is increased threefold, and ED is positively correlated with metabolic syndrome, hypertension, and dyslipidemia and negatively correlated with better glycemic control and physical activity. ED predicts CAD events in diabetic men with no evidence of CAD and major adverse cardiac events in men with type 2 diabetes who have established, asymptomatic CAD (hazard ratio 2.1, p <0.001). In obese men, ED is correlated with endothelial dysfunction, decreased NO production, and increased proinflammatory cytokines, body mass index, and waist/hip ratio. In 110 obese men without diabetes, ED was strongly correlated with waist/hip ratio and was significantly improved with weight loss and increased activity, which reduced glucose, insulin, waist/hip ratio, blood pressure, and triglycerides and increased endothelial NO production. In obese men on a program of diet and vigorous activity, increased insulin sensitivity, manifested by reduced circulating insulin, was correlated with increased NO production (r = 0.83).
Hypertension
The prevalence of ED is 2 to 3 times higher in men with hypertension without diabetes or other medical conditions, and the incidence of ED increases with the duration and severity of elevated blood pressure. ED predicts a doubling of the risks of myocardial infarction and cardiac death in hypertensive men. Antihypertensive medications generally adversely affect erectile function but short-acting angiotensin II receptor blockers significantly improved coital frequency in men without ED (valsartan) and erectile function in men with ED and metabolic syndrome (irbesartan). In a randomized, double-blind, crossover study of men with type 2 diabetes and hypertension, the angiotensin II receptor blocker losartan caused a significant increase of flow-mediated dilation compared to an angiotensin-converting enzyme inhibitor (p = 0.01) and also significantly decreased a marker of oxidative stress (p <0.001).
Omega-3 Fatty Acids
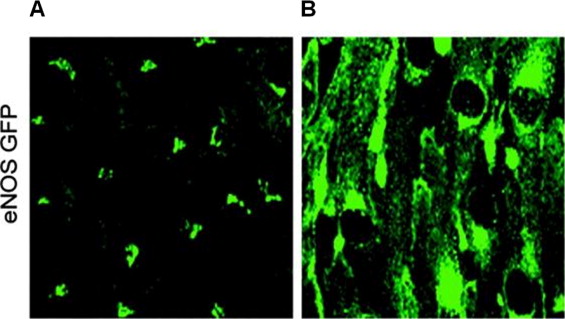
Omega-3 fatty acids, obtained in the diet from fatty fish such as salmon, herring, and sardines, commercially as fish oil capsules, or by prescription (omega-3 acid ethyl esters), promote vascular health and reduce the risk for sudden cardiac death by their anti-inflammatory, antiarrhythmic, and platelet antiaggregation effects, by reducing circulating triglycerides and by stimulating the release of NO. Eicosapentaenoic acid, 1 of the 2 main omega-3 fatty acids, rapidly increases the production of NO in human endothelial cells ( Figure 2 ) and also prevents the decrease of NO caused by glucose. These findings support using eicosapentaenoic acid to enhance erectile function and indicate that some of the benefits ascribed to omega-3 fatty acids are manifested through increased NO. Because the American Heart Association recommends 1,000 mg of omega-3 fatty acids daily for patients with established CAD, 500 to 1,000 mg is a reasonable daily intake to maximize erectile and vascular health. These levels are “generally recognized as safe” by the United States Food and Drug Administration.
Antioxidants
Reduced glutathione is the most important cellular antioxidant and an essential cofactor for NOS. In nondiabetic men, the mean ± SD intracellular level of red blood cell reduced glutathione was significantly lower in men with ED (1,932 ± 581 μmol/L) compared to men with normal erectile function (2,269 ± 232 μmol/L) (p <0.001). The reduced glutathione levels were lowest in men with ED and diabetes, to 1,671 ± 438 μmol/L, a level significantly lower than with diabetes alone (2,084 ± 118 μmol/L) (p <0.001). These lower levels suggest that men with ED are deficient in dietary antioxidants that help keep glutathione in the reduced state and/or that oxidative stress associated with poor lifestyle choices and vascular diseases compromises cellular antioxidant defenses in these men.
Pomegranate, chocolate, blueberries, green tea, and red wine contain high levels of polyphenolic antioxidants and increase NO in animal and human in vitro and in vivo studies. Antioxidants promote NO synthesis and oppose NO degradation. Chocolate consumption and tea consumption have each been associated with reduced mortality after an initial myocardial infarction. Because foods high in antioxidants such as dark chocolate usually have a bitter taste, commercial products often contain sugar. Sugar markedly reduces the positive effects of cocoa on vascular NO production ( Figure 3 ). Ginseng and Pycnogenol (Horphag Research and Natural Health Science, Hoboken, New Jersey) are 2 nonprescription antioxidants that improved erectile function in randomized, double-blind, placebo-controlled, crossover trials in which sugar intake was not a confounder.

Folic Acid
Folic acid increases NOS, and deficient dietary intake is common. The United States Food and Drug Administration recommended daily allowance is 400 μg. However, because of an unresolved controversy regarding whether folic acid supplementation could stimulate established colorectal or other cancers, caution is prudent regarding folic acid supplementation when dietary intake is adequate.
Calcium
Physiologic changes of calcium levels modulate the synthesis of NO by vascular endothelium. A meta-analysis of 40 randomized trials of calcium supplementation showed a small but significant decrease of blood pressure, the effect being greater in subjects with insufficient dietary intake. Calcium intake should not exceed 1,500 mg/day, because high calcium intake is associated with more advanced and aggressive prostate cancers. Recommended calcium intake also should not be exceeded because calcium supplementation in women already ingesting >800 mg/day has been associated with myocardial infarction.
Vitamins C and E
The antioxidant potency of vitamins C and E is 30 to 50 times lower than the polyphenols listed previously. Ascorbic acid increases eNOS bioactivity and NO production in a variety of disease states. Some studies of vitamin E in humans and many in animals have shown increased NO levels and beneficial effects on vascular function. Vitamins C and E have synergistic effects on serum levels achieved after ingestion. Vitamin E should be limited to ≤200 IU/day because of a reported increase in all-cause mortality with higher doses and hemorrhagic stroke in physicians given 400 IU every other day. Many older men take low-dose aspirin, and vitamin E markedly potentiates the antiplatelet effect of aspirin in response to collagen in vitro. Although all antioxidants may potentiate the antiplatelet effect of aspirin through stimulation of NO, vitamin E supplements are better avoided when taking aspirin. Maximizing NO production may provide cardioprotective effects similar or superior to aspirin without its associated risks, particularly when aspirin is used as primary prevention, whereby the risk for major bleeding may counterbalance the reduction of cardiovascular events.
l -Arginine and l -Citrulline
l -Arginine is the precursor of NO and has been investigated to boost NO production. However, oral l -arginine is metabolized by arginase in the gut wall and liver, and the major source of l -arginine within the endothelial cell is from l -citrulline. The 2 amino acids increase vascular NO production and reduce atherosclerosis in rabbits ingesting an atherogenic diet. However, for the treatment of ED with l -arginine, randomized trials have shown no benefit using 1.5 g/day, with 5 g/day required to detect any improvement.
Oral l -citrulline increases l -arginine levels more effectively than oral l -arginine, with 1.5 g/day of l -citrulline increasing levels to a similar degree as 3.2 g/day of oral l -arginine. These studies indicate that 5 g of l -arginine or 2 to 3 g of l -citrulline may benefit ED. However, NO is also involved in inflammatory responses through inducible NOS. The finding in 1 study that 9 g/day of l -arginine appeared to increase mortality with acute myocardial infarction strongly suggests that the administration of high doses of l -arginine or l -citrulline during acute inflammatory events could have serious consequences.
Testosterone
An association exists between male hypogonadism and the metabolic syndrome, and testosterone treatment can reduce central adiposity and insulin resistance. The circulating level of testosterone correlates with vascular NO production, and testosterone replacement in hypogonadal men with ED improves erectile function.
Smoking
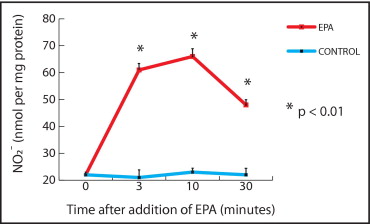
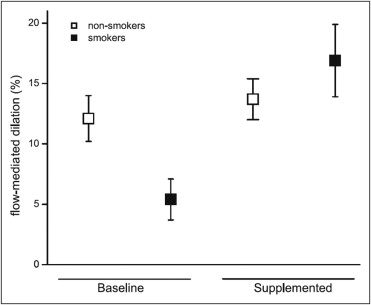
Smoking doubles the risk for ED, and secondhand smoke also increases the risk for ED. Smoking and cigarette smoke extract reduce NO in vitro and in vivo through oxidative stress (the generation of superoxide and peroxynitrite). Uncoupling of eNOS results in increased production of superoxide and conversion of NO to peroxynitrite. Peroxynitrite is a potent pro-oxidant that reduces eNOS bioactivity. Antioxidant supplements can recouple eNOS and protect NO from destruction by superoxide. The effect of smoking on NO was completely reversed by high daily doses of vitamins C (1,000 mg) and E (800 IU) ( Figure 4 ).
Alcohol
Mild to moderate alcohol consumption is associated with less ED (odds ratio 0.79, 95% confidence interval 0.67 to 0.92, p <0.001), in part because of favorable effects on high-density lipoprotein levels. Moderate alcohol consumption also increases eNOS and NO in laboratory animals. Excessive alcohol, however, suppresses endothelial function. In the corpus cavernosum of the mouse, alcohol reduced endothelial (but not neural) NO release and induced structural changes in the endothelium.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


