FIGURE 11-1 Learning curve: procedure failure rate, sheath insertion delay, and procedure duration. (From Spaulding C, Lefevre T, Funck F, et al. Left radial approach for coronary angiography: results of a prospective study. Cathet Cardiovasc Diagn. 1996;39(4):365–370.)
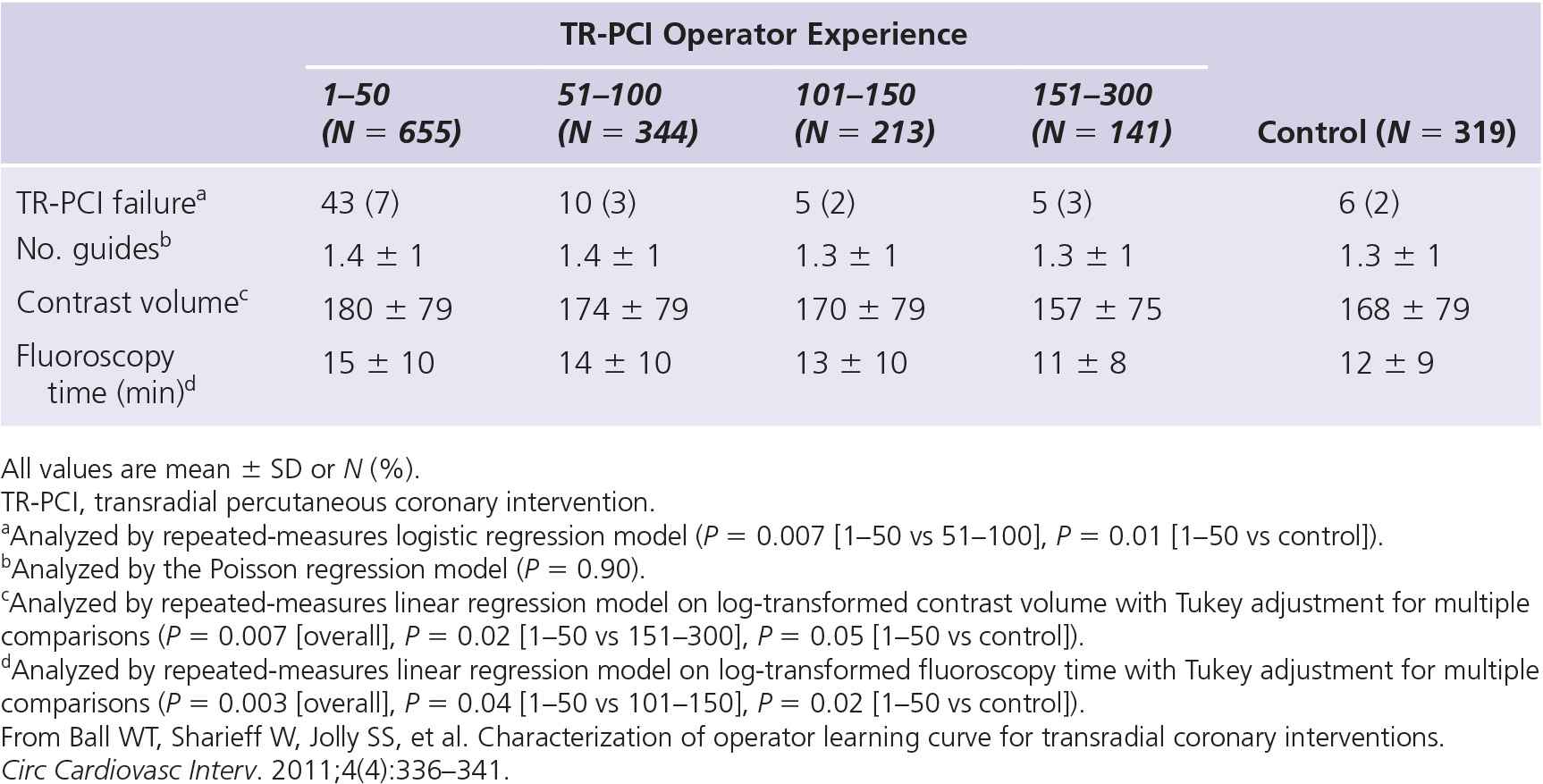
TABLE 11-1 Procedural Outcomes
The Learning Curve of Transradial Angiography and Intervention for Novice Operators
The previously discussed studies mostly dealt with the learning curve of radial access among experienced femoral operators. The preferable method for training new interventional fellows in radial access is not well studied. Should they initially focus on femoral access and once comfortable with this approach, move on to radial procedures? Or is it preferable to train in both access routes in a parallel manner? A study presented at TCT 2011 by Javed et al.15 looked at procedure performance indices of interventional cardiology fellows during their first year of training. A total of 1,777 coronary catheterizations were performed (34% of procedures were PCI). Of these, 19% were done via the radial route. The authors reported high procedure success rates (95.6% for radial access and 99.9% for femoral access). There was no difference in procedure time, fluoroscopy time, or contrast use between radial and femoral routes. On comparing the radial procedures performed in the first six months versus the second six months, there was a significant reduction in all measured indices.
The Implication of Transradial Learning Curve for Training and Competency Guidelines
There are no clear recommendations or consensus on the period of training or the number of cases required to be proficient in transradial coronary procedures, although recommendations from Society for Cardiovascular Angiography and Interventions (SCAI) and ESC have been published recently (Fig. 11-2). In the United States, to be eligible for certification by the American Board of Internal Medicine, each trainee needs to perform a minimum of 250 PCI procedures during training, but no specific recommendations are provided in terms of radial access.16 The ACC Core Cardiology Training Symposium (COCATS) guidelines recommend that trainees need to be able to “perform vascular access from the femoral, radial, or brachial route,” but do not provide criteria or guidelines for competency in transradial procedures. The curriculum and syllabus for interventional cardiology subspecialty training in Europe recommends trainees learn “vascular access, including principles of femoral, radial and brachial procedures,” with no further recommendations on recognizing competence in transradial procedures. The SCAI has recognized and called for the need of formalizing transradial PCI training. The SCAI has also proposed a three-tiered competency classification17 as follows:
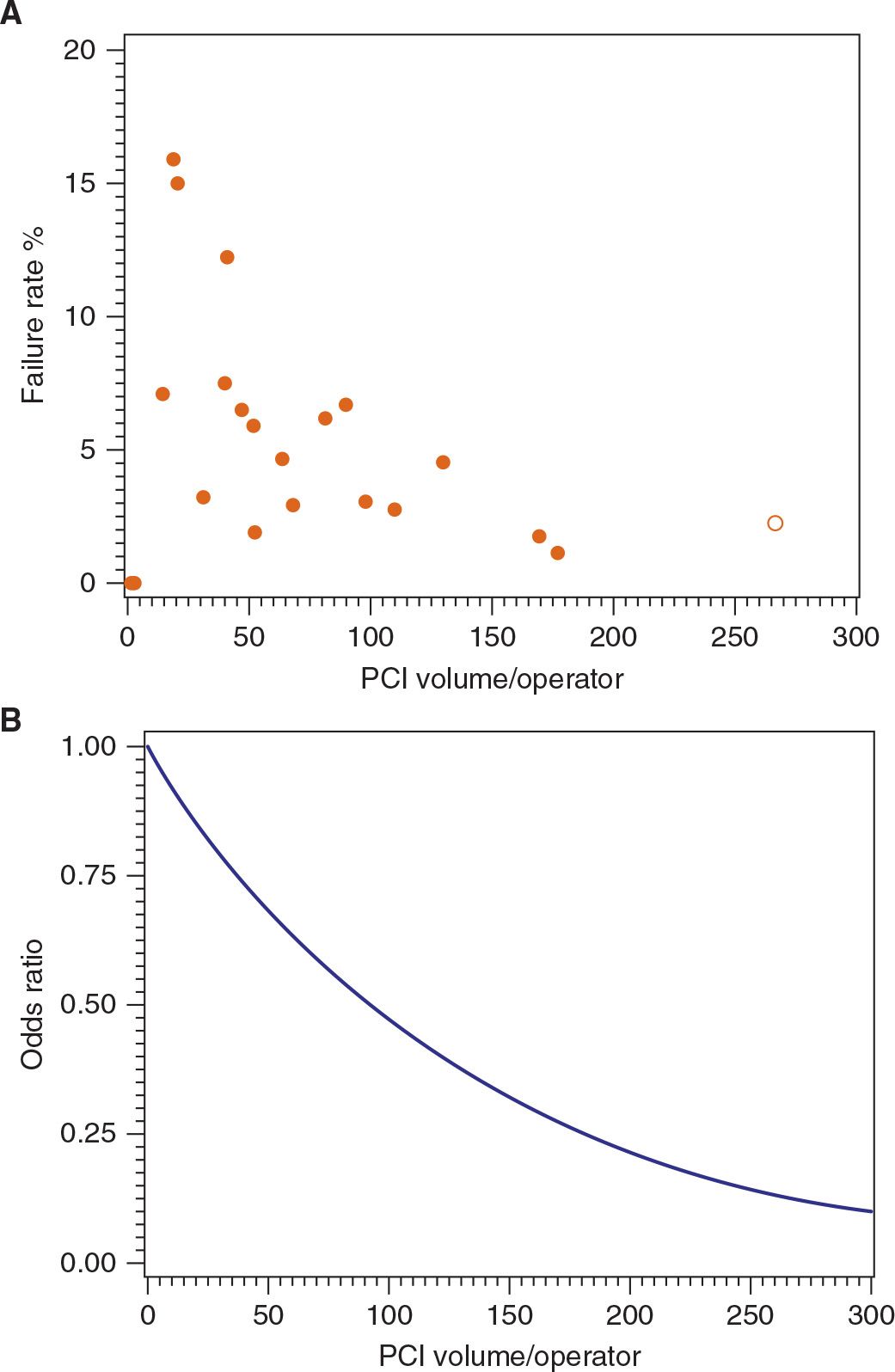
FIGURE 11-2 Relationship between TR-PCI volume and failure rate. A: Data for individual operators are shown. Solid circles represent individual TR-PCI operators for four experience groups and the open circle represents the control group shown as a reference. Case volume was defined as total cases performed by individual operators in the four experience groups and total cases performed by all operators in the control group. B: Data illustrated as odds ratios of failure to total TR-PCI volume. The results of logistic regression analysis showed that the relative odds of TR-PCI failure decline substantially up to 50 cases, and further decline after 100 cases is small. PCI, percutaneous coronary intervention; TR-PCI, transradial percutaneous coronary intervention. (From Ball WT, Sharieff W, Jolly SS, et al. Characterization of operator learning curve for transradial coronary interventions. Circ Cardiovasc Interv. 2011;4(4):336–341.)
• Level 1 competency: Able to perform simple diagnostic cases on patients with favorable upper limb anatomy (large men).
• Level 2 competency:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


