Fig. 13.1
Transeosophageal echocardiographic still frame shows evidence of small atrial communication on 2D and turbulent flow on colour mapping
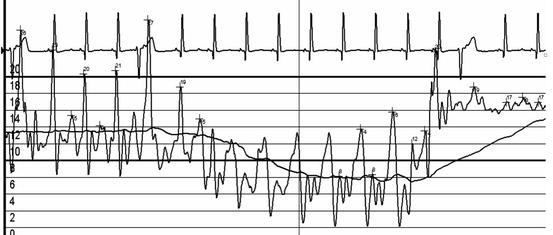
Fig. 13.2
Haemodynamic pressure tracing shows a reproducible pressure gradient during pullback of a multitrack catheter over a wire (left to right on figure) from pulmonary vein to left atrium to right atrium then through the fenestration into the Fontan conduit
The fenestration was crossed from the femoral vein and a stable wire position was secured in the left lower pulmonary vein. A large Genesis stent mounted onto a 16-mm balloon was placed via a 10 French long sheath, with abolition of the trans-atrial gradient (Fig. 13.3). The fenestration was also enlarged by a separate, short stent. Final Fontan pressure was 15 mmHg and saturations were 89 %. Pleural drainage stopped over the next 48 h, the patient was discharge day 6 post catheterization. At 16 month follow-up, saturations were 90 % and exercise tolerance was satisfactory.
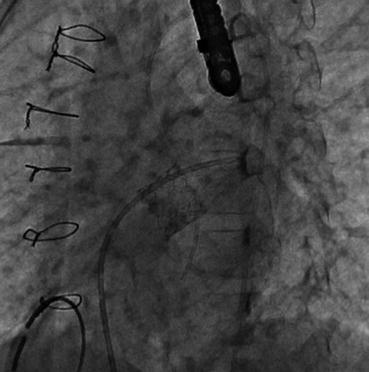
Fig. 13.3
Fluroscopic still shows the large Genesis stent in place across the atrial septum
The Fontan Circulation
The Fontan circulation results in a ‘neo-portal’ system; systemic venous blood is re-routed directly to the pulmonary arteries, bypassing the ventricular pump. Trans-pulmonary flow is driven solely by the pressure gradient between systemic veins and receiving ventricle. For the majority, this gradient is dictated by relatively fixed resistance across the pulmonary capillary bed. Due to the infant’s pulmonary vascular resistance (PVR) being relatively high, successful total cavopulmonary connection must be performed in a staged fashion.
Initial surgical palliation secures an adequate outlet for systemic arterial flow and a systemic to pulmonary arterial shunt for pulmonary blood flow. At this stage, ventricle pre-load is high due to shunt return, and complete mixing means saturations are low. Superior caval venous return is surgically connected to the pulmonary arteries in the first 4–12 months of life with the ‘bidirectional cavopulmonary shunt’ (a modification on the original ‘Glenn procedure’,) and the shunt is taken down. Cyanosis persists at this stage, but ventricular pre-load is restored to near physiological levels. Inferior caval blood is later connected to the pulmonary arteries with a conduit or baffle, completing the Fontan circuit. (See Fig. 13.4 for a schematic overview of the staged circulations). Once the Fontan circuit is complete, no systemic venous blood enters the heart, achieving normal systemic oxygen saturation.
Fig. 13.4
(a) Normal biventricular circulation. Pulmonary circulation (P) is connected with the systemic circulation (S) via the right ventricle. The right ventricle maintains right atrial pressure lower than left atrial pressure, and provides enough energy for the blood to pass through the pulmonary resistance. (b) Arterially shunted palliation. The systemic (S) and pulmonary (P) circuits are connected in parallel, with a considerable volume overload to the single ventricle. There is complete admixture of systemic and pulmonary venous blood, causing arterial oxygen desaturation. (c) Fontan circuit. Systemic veins (V) are connected to the pulmonary artery, without a sub-pulmonary ventricle or systemic atrium. The lungs are thereby converted into a neo-portal system, which limits flow to the ventricle. In the absence of a fenestration, there is no admixture of systemic and pulmonary venous blood. Ao aorta, CV caval veins, F fenestration, LA left atrium, LV left ventricle, PA pulmonary artery, RA right atrium, RV right ventricle, V single ventricle. Line thickness reflects output (Reproduced from Heart, The Fontan circulation, Gewillig M, 91(6), 839–846, Copyright 2005, with permission from BMJ Publishing Group Ltd.)
In 1977, Choussat described ten criteria for the ideal Fontan candidate (Table 13.1). Though these remain desirable, most of these ‘commandments’ have since been broken. However, it is crucial that the pulmonary arteries must be large enough to receive a conduit adequate for adulthood and the PVR must have fallen adequately. Completion is typically performed between the ages of 3 and 5 years. Operating centre experience and clinical criteria, such as oxygen saturation and exercise tolerance, usually govern timing.
Table 13.1
Choussat’s 1977 selection criteria for identifying the ideal Fontan candidate (frequently referred to as ‘The Ten Fontan Commandments’a)
Age >4 years |
Sinus rhythm |
Normal systemic venous return |
Normal right atrial volume < div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|