(1)
Anatomy Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania
Abstract
Classically, the heart size is compared to the size of the right wrist of the individual. This comparison is more suggestive than true, the heart size varying with the constitutional type, age, physiological status and possible pathology (Fig. 4.1) 1.
4.1 The General Presentation
Classically, the heart size is compared to the size of the individual’s right fist. This comparison is more suggestive than true, the heart size varying with the constitutional type, age, physiological status and possible pathology (Fig. 4.1).

Fig. 4.1
Ventricular pyramids of different size
Accordingly to the classical view, the heart presents a sternocostal surface, a pulmonary surface, a diaphragmatic surface, a right border, a base and an apex.
The sternocostal surface is named that way because of its relation with the sternum and the ribs (Figs. 4.2–4.10).
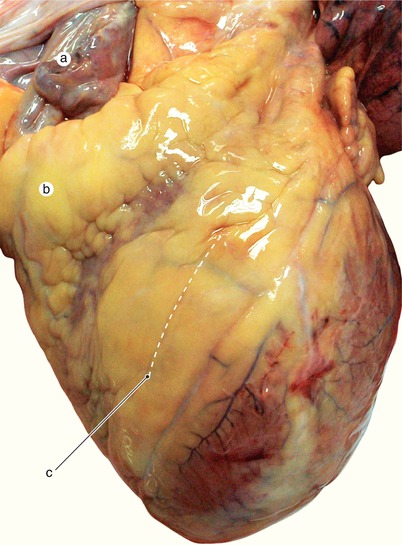
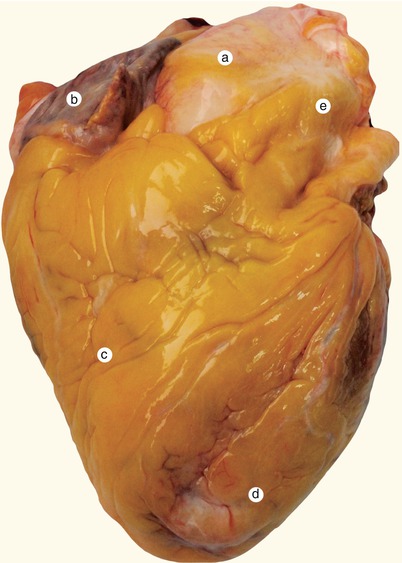
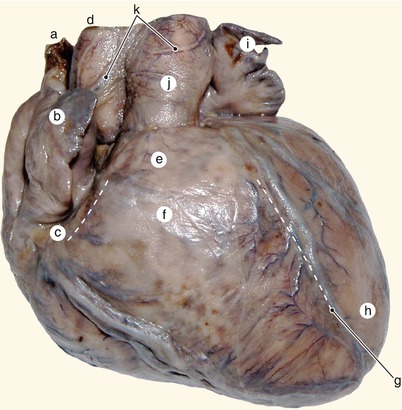
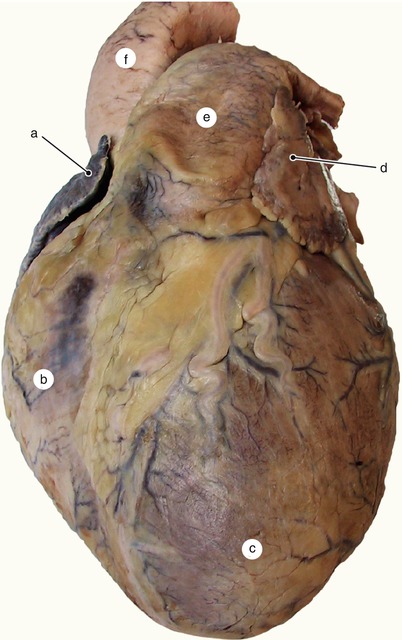
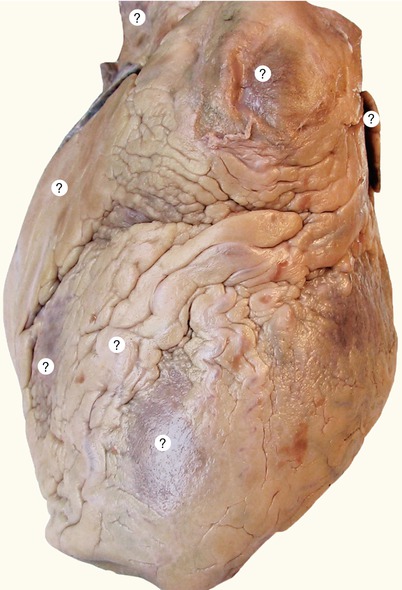
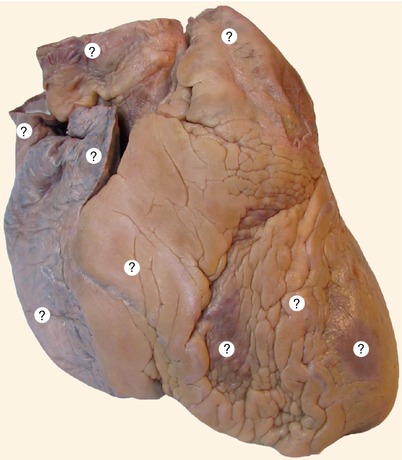
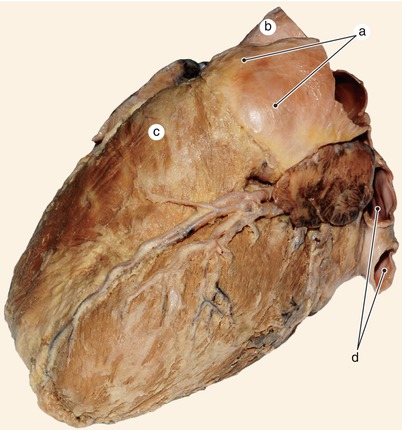
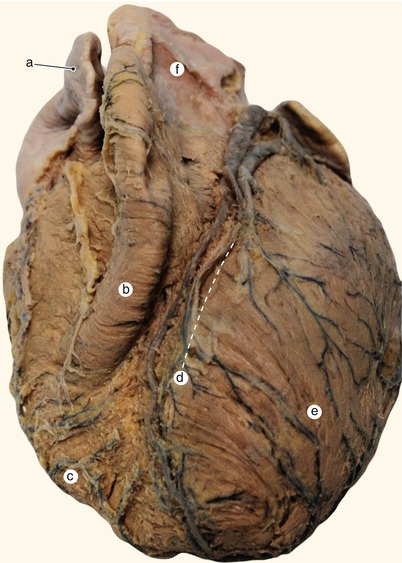
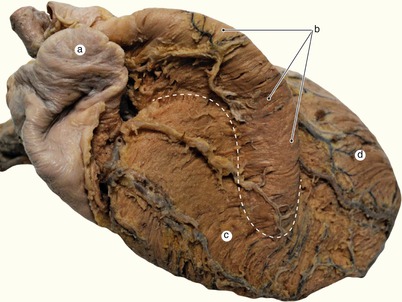
Fig. 4.2
Non-formaldehyded heart. Notice the different consistence of the atrial wall (flaccid) in comparison with the ventricular one (firm). a Right atrium, b fat deposits in the right coronary groove, c positioning of the anterior interventricular groove
Fig. 4.3
Non-formaldehyded heart. Massive subepicardic fat accumulation. a Ascending aorta, b right atrium, c right ventricle, d left ventricle, e pulmonary trunk
Fig. 4.4
Fetal heart of 7 months of age. Notice the total absence of subepicardic fat deposits. a Superior vena cava, b right auricle, c right coronary groove, d aorta, e right ventricle’s infundibulum, f right ventricle’s conus, g anterior interventricular groove, h left ventricle, i left auricle, j pulmonary trunk, k periarterial nervous plexus
Fig. 4.5
Formaldehyde prepared heart. The fat depositing usually met in healthy individuals. a Right auricle, b right ventricle, c left ventricle, d left auricle, e pulmonary trunk, f ascending aorta
Fig. 4.6
Undissected heart. Plese identify the structers on the sterno-costal surface (same as the Fig. 4.5)
Fig. 4.7
Undissected heart. Plese identify the structers on the right surface (same as the Fig. 4.4)
Fig. 4.8
The well structured subpulmonary infundibulum continues with an evident bulb at the origin of the pulmonary artery. a Pulmonary trunk’s bulb, b aorta, c subpulmonary infundibulum, d left pulmonary veins
Fig. 4.9
The bulbus cordis from the embryological period kept the individuality of the conal region. The conus projects on the sternocostal surface like a well structured formation. a Right auricle, b conal region, c right ventricle, d anterior interventricular groove, e left ventricle, f pulmonary trunk
Fig. 4.10
The conus has its own vessels an presents a specific myocardial organization. The dotted line represents the conal limits. a Right auricle, b former region of the ventricular bulbus, currently the conoinfundibular region, c right ventricle, d left ventricle
At this surface the atria are partially visible (in the superior one-third) but also the ventricles participate (in the inferior two-thirds). The ventricular component is represented in most of its part by the right ventricle and the rest by the left ventricle, the two ventricles being separated by the anterior interventricular groove (we say that the right heart is situated anteriorly to the left one). In this groove (in general at its left side) passes the anterior interventricular artery and the great cardiac vein. The groove finishes at about 1–2 cm to the right of the cardiac apex, inducing the appearance of the apexian notch at the right border of the heart. Its depth is highly variable.
The apex of the heart is orientated towards inferior and to the left and represents the region comprising both ventricles, separated by the apexian notch. Its appearance is variable and will be treated in detail+-z\z\ to the general architecture of the myocardium chapter.
The right ventricle extends superiorly and to the left with a region which presents an aspect compared with a truncated cone named the pulmonary conus. This region continues with an almost cylindrical segment with a variable presence and aspect, named the pulmonary infundibulum. Its distal part is the subvalvar infundibulum which finishes at the pulmonary valve as the last segment of the right ventricle having a muscular wall. Beyond the pulmonary valve, the right ventricle continues with the pulmonary trunk.
The atrial component of the sternocostal surface remains mostly hidden behind the emergence of the two great arteries, the aorta and the pulmonary artery.
The atria are separated from the ventricles by an anteriorly incomplete circular groove, the coronary groove. In its right side, the coronary groove contains the right coronary artery and the small cardiac vein, while its left side contains the circumflex artery, the great cardiac vein and the coronary sinus.
Towards the base of the heart, on the sternocostal surface, there are two arterial projections named the right and the left auricles. The auricles covers the anterior extremities of the atrio-ventricular groove and looks like it covers the origin of the two great vessels, the aorta and the pulmonary trunk. The whole ensemble is known as the “corona cordis”. Inside the corona cordis, the aorta is situated to the right and posterior while the pulmonary artery to the left and anterior. These vessels give the impression that twist one inaround each other (Figs. 4.11, 4.12 and 4.13).
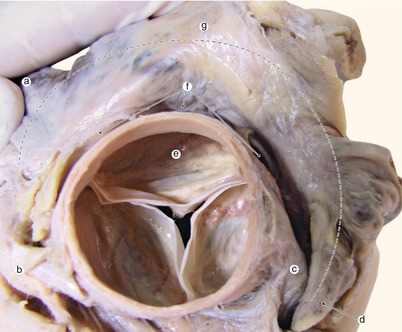
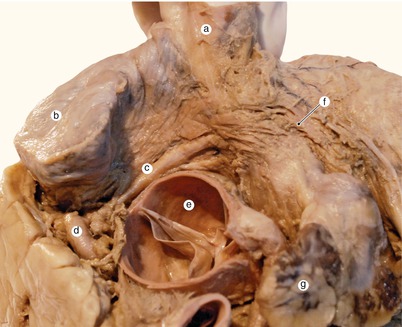
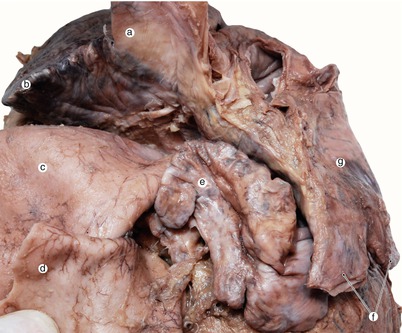
Fig. 4.11
Interatrial notch and corona cordis. a Right auricle between examiner’s fingers, b right coronary artery, c left coronary artery, d left auricle, e aorta, f transverse pericardial sinus located behind the aorta, g. corona cordis
Fig. 4.12
The interatrial notch and a variant of the sinoatrial node artery. a Superior vena cava, b right auricle, c sinoatrial node artery, d right coronary, e aorta, f interatrial fasciculus
Fig. 4.13
The left auricle is prominent retroaortic. a Superior vena cava, b right auricle, c aorta, d pulmonary trunk, e left auricle, f left pulmonary veins, g left atrium
The pulmonary surface is represented by a large portion of the left ventricle (Figs. 4.14, 4.15, 4.16, 4.17, 4.18, 4.19, 4.20 and 4.21). This surface also presents the name of the obtuse border of the heart (margo obtusis). The name of pulmonary surface occurs due to the intimate relation with mediastinal surface of the left lung which marks the cardiac impression (inferior to the hilum).
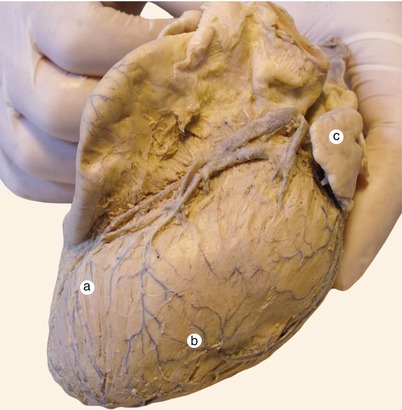
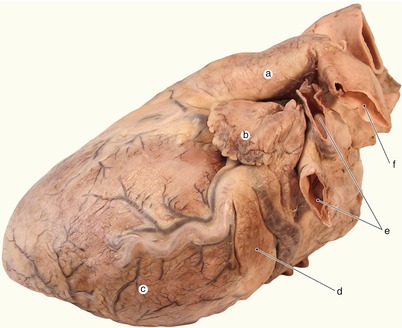
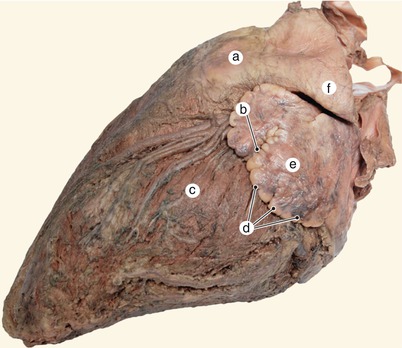
Fig. 4.14
Between the pulmonary and the sternocostal faces there is no precise limit. a Sternocostal face left ventricle, b pulmonary face left ventricle, c left auricle
Fig. 4.15
Notice on the pulmonary surface, towards the ventricular base, the existence of an individualized ventricular muscle fasciculus. a Pulmonary trunk, b left auricle, c pulmonary surface of left ventricle, d ventricular muscle fasciculus, e pulmonary veins, f left pulmonary artery
Fig. 4.16




The left auricle has crenelate borders and deep notches that completely separate unequal territories. a Pulmonary trunk, b auricular notch, c pulmonary face left ventricle, d crenelate border left auricle, e left auricle, f left pulmonary artery
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
