7
The Effects of Other Conditions on the ECG
The ECG is not a good method for investigating or diagnosing any condition that is not primarily cardiac. However, some generalized diseases do affect the ECG: it is important to recognize this, and not assume that a patient has heart disease simply because their ECG seems abnormal.
ARTEFACTS IN ECG RECORDINGS
THE EFFECTS OF ABNORMAL MUSCLE MOVEMENT
Sustained involuntary tremors, such as those associated with Parkinsonism ( Fig. 7.1) cause rhythmic ECG abnormalities that may be confused with cardiac arrhythmias.

HYPOTHERMIA
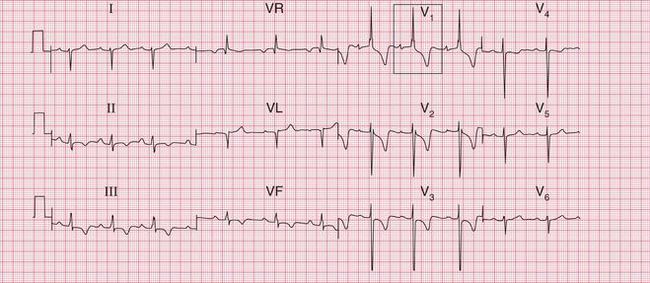
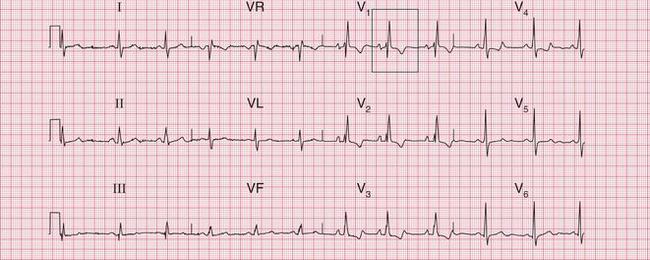
Hypothermia causes shivering, and therefore artefacts due to muscular activity. However, there can be other changes in the ECG, and the characteristic ECG feature of hypothermia is the ‘]’ wave. This is a small hump seen at the end of the QRS complex ( Fig. 7.2).
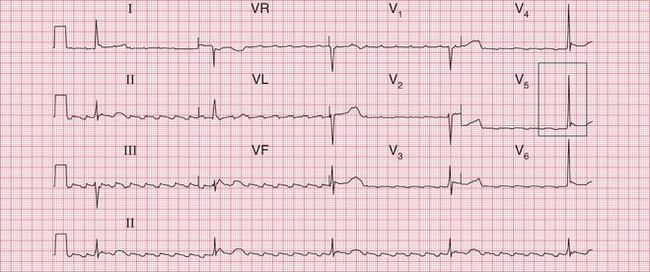

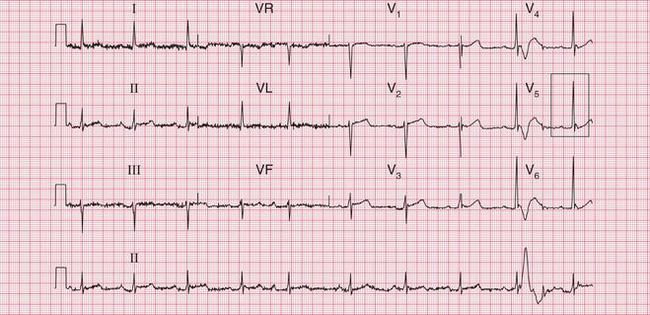
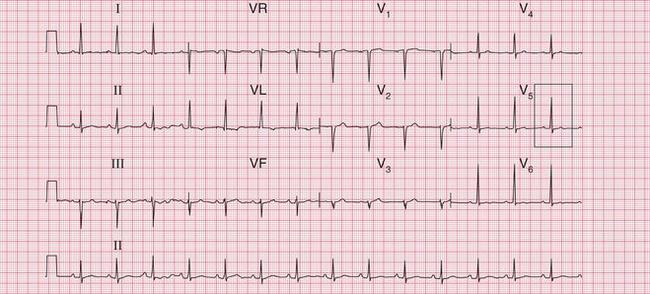
The ECG in Figure 7.2 was recorded from a 76-year-old woman who was admitted to hospital with a temperature of 30°C after lying for a prolonged period in a freezing house, after a fall. She initially had a heart rate of 26/min, and the rhythm was atrial flutter. J waves can be seen in the lateral chest leads. On re-warming, she began to shiver, and, despite the muscle artefact, her heart can be seen to have reverted to sinus rhythm with first degree block. J waves are still visible ( Fig. 7.3). When her temperature had returned to normal, the PR interval normalized and the J waves disappeared ( Fig. 7.4).

THE ECG IN CONGENITAL HEART DISEASE
The ECG provides a limited amount of help in the diagnosis of congenital heart disease by showing which chambers of the heart are enlarged. It is important to remember (see Ch. 1) that at birth the ECG of a normal infant shows a pattern of ‘right ventricular hypertrophy’, and this gradually disappears during the first 2 years of life.
Box 7.1 lists some common congenital disorders and the associated ECG appearances.
The ECG in Figure 7.5 shows all the features of severe right ventricular hypertrophy: it came from a boy with severe pulmonary stenosis.

The ECG in Figure 7.6 shows left ventricular hypertrophy, and was recorded in an 8-year-old with severe aortic stenosis.
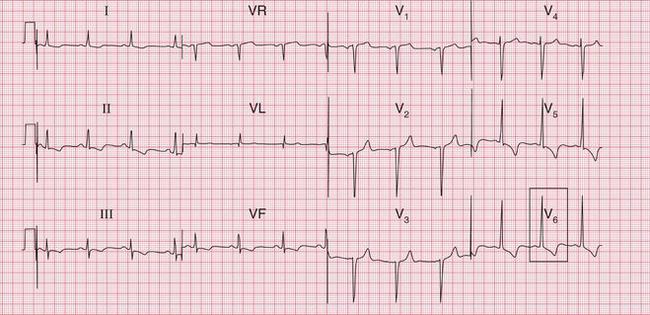

Fig. 7.6 Left ventricular hypertrophy
Note
The ECG in Figure 7.7 shows right ventricular hypertrophy, and came from a young woman who had had a partial correction of Fallot’s tetralogy 20 years previously.
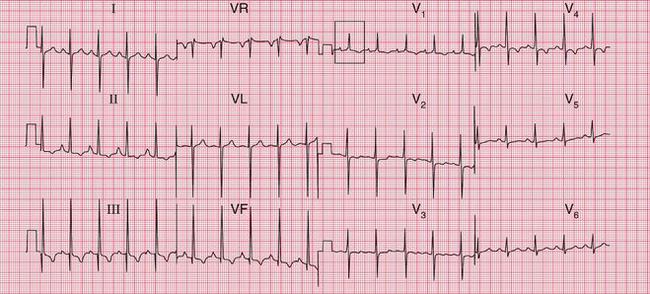

Fig. 7.7 Right ventricular hypertrophy in Fallot’s tetralogy
Note
The ECG in Figure 7.8 suggests right atrial hypertrophy and shows right bundle branch block. It came from a teenager with Ebstein’s anomaly and an atrial septal defect.
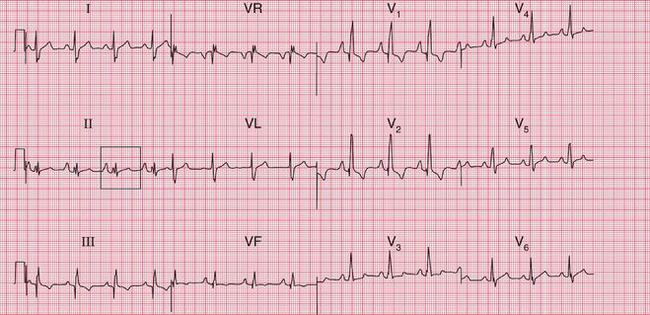

Fig. 7.8 Right atrial hypertrophy and right bundle branch block, in Ebstein’s anomaly
Note
It is usually fairly obvious that a patient has congenital heart disease of some sort, but the condition that may be missed is an atrial septal defect. The ECG in Figure 7.9 is from a 50-year-old woman who complained of mild but increasing breathlessness. She had a rather nonspecific systolic murmur at the left sternal edge. Her GP recorded an ECG which showed right bundle branch block, and as a result she had an echocardiogram which showed an atrial septal defect.

THE ECG IN SYSTEMIC DISEASES
THYROID DISEASE
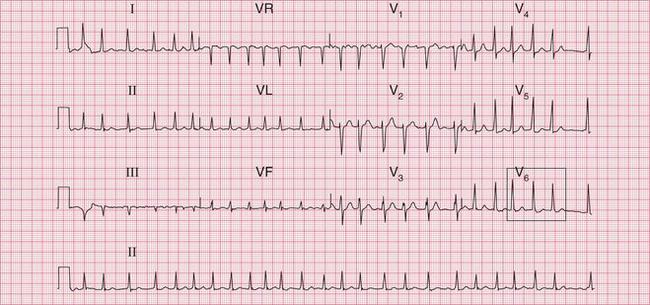
Thyrotoxicosis is probably the most common non-cardiac disorder that may present as a cardiac problem. It may cause atrial fibrillation, particularly in old age. There is usually a rapid ventricular response, which is difficult to control with digoxin ( Fig. 7.10). An elderly patient may complain of palpitations or the symptoms of heart failure, and arterial embolization may occur. The usual symptoms of thyrotoxicosis may be mild or even absent.

< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


