3
The ECG When the Patient has a Tachycardia
Enhanced automaticity and triggered activity
Abnormalities of cardiac rhythm due to re-entry
Differentiation between re-entry and enhanced automaticity
Extrasystoles causing symptoms
Narrow complex tachycardias causing symptoms
Broad complex tachycardias causing symptoms
Special forms of ventricular tachycardia in patients with symptoms
Tachycardias associated with the Wolff–Parkinson–White syndrome
What to do when an arrhythmia is suspected
What to do when an arrhythmia is recorded
Atrioventricular nodal re-entry tachycardia (AVNRT, junctional tachycardia)
Atrial fibrillation and flutter
The Wolff–Parkinson–White syndrome
Electrophysiology and catheter ablation
Arrhythmias amenable to ablation
Indications for electrophysiology
The only tachycardia that can be (reasonably) reliably diagnosed from the patient’s history is sinus tachycardia. A patient may notice the irregularity of atrial fibrillation, but it is easy to confuse this with multiple extrasystoles. The heart rate may give a clue to the nature of the arrhythmia ( Table 3.1) but there is really no substitute for the ECG.
Table 3.1
Physical signs and arrhythmias
| Pulse | Heart rate (beats/min) | Possible nature of any arrhythmia |
| Arterial pulse | ||
| Regular | < 50 | Sinus bradycardia |
| Second or third degree block | ||
| Atrial flutter with 3 : 1 or 4 : 1 block | ||
| Idionodal rhythm (junctional escape), with or without | ||
| sick sinus syndrome | ||
| 60-140 | Probable sinus rhythm | |
| 140-160 | Sinus tachycardia or an arrhythmia | |
| 150 | Probable atrial flutter with 2 : 1 block | |
| 140-170 | Atrial tachycardia | |
| Atrioventricular re-entry tachycardia (AVRT) | ||
| Atrioventricular nodal re-entry tachycardia (AVNRT; | ||
| junctional (nodal) tachycardia) | ||
| Ventricular tachycardia | ||
| > 180 | Probable ventricular tachycardia | |
| 300 | Atrial flutter with 1 : 1 conduction | |
| Irregular | Marked sinus arrhythmia | |
| Extrasystoles (supraventricular or ventricular) | ||
| Atrial fibrillation | ||
| Atrial flutter with variable block | ||
| Rhythm varying between sinus rhythm and any arrhythmia or conduction defect | ||
| Jugular venous pulse | ||
| More pulsations visible than heart rate | Second or third degree block | |
| Cannon waves – third degree block |
MECHANISM OF TACHYCARDIAS
ENHANCED AUTOMATICITY AND TRIGGERED ACTIVITY
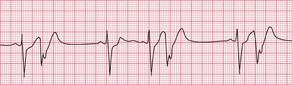
If the intrinsic frequency of depolarization of the atrial, junctional or ventricular conducting tissue is increased, an abnormal rhythm may occur. This phenomenon is called ‘enhanced automaticity’. Single early beats, or extrasystoles, may be due to enhanced automaticity arising from a myocardial focus. The most common example of a sustained rhythm due to enhanced automaticity is ‘accelerated idioventricular rhythm’, which is common after acute myocardial infarction. The ECG appearance ( Fig. 3.1) resembles that of a slow ventricular tachycardia, and that is the old-fashioned name for this condition. This rhythm causes no symptoms, and should not be treated.

If the junctional intrinsic frequency is increased to a point at which it approximates to that of the SA node, an ‘accelerated idionodal rhythm’ results. This may appear to ‘overtake’ the P waves ( Fig. 3.2). This rhythm used to be called a ‘wandering pacemaker’. The term ‘focal junctional tachycardia’ is used in the (probably rare) instances of a supraventricular tachycardia originating around the AV node, by mechanisms other than re-entry.

‘Triggered activity’ results from late depolarizations which occur after normal depolarization, during what would normally be a period of repolarization. Like enhanced automaticity, this can cause extrasystoles or a sustained arrhythmia, such as right ventricular outflow tract ventricular tachycardia (RVOT-VT) ( Fig. 3.3).
ABNORMALITIES OF CARDIAC RHYTHM DUE TO RE-ENTRY
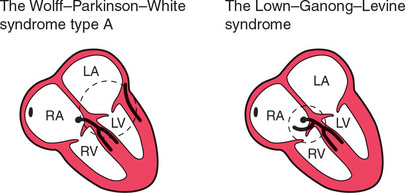
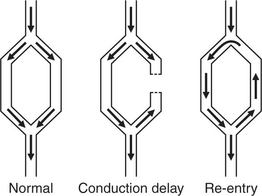
Normal conduction results in the uniform spread of the depolarization wave front in a constant direction. Should the direction of depolarization be reversed in some part of the heart, such as in an accessory connection between the atria and ventricles, it becomes possible for a circular or ‘re-entry’ pathway to be set up. Activation travels round and round the circuit, causing a tachycardia such as the atrioventricular reentry tachycardia (AVRT) experienced by patients with the Wolff-Parkinson-White (WPW) syndrome or the Lown-Ganong-Levine (LGL) syndrome ( Fig. 3.4).
ATRIOVENTRICULAR RE-ENTRY TACHYCARDIA (AVRT)
In the pre-excitation syndromes, normal and accessory pathways between an atrium and a ventricle together form an anatomical circuit round which depolarization can reverberate, causing a ‘re-entry’ tachycardia ( Fig. 3.5). Once established, a circular wave of depolarization will continue until some part of the pathway fails to conduct. Alternatively, the circular wave may be interrupted by the arrival of another depolarization wave, set up by an ectopic focus (e.g. an extrasystole).
In the WPW syndrome, the re-entry circuit comprises the normal AV node-His bundle connection between the atria and the ventricles, and an accessory pathway, the bundle of Kent, which also connects the atria and ventricles, bypassing the AV node ( Fig. 3.4). If forward conduction in the accessory pathway is blocked, depolarization can spread down the normal pathway and back (i.e. retrogradely) via the accessory pathway, to reactivate the atria. Recurrent activation of the circuit can cause a ‘circus movement’, resulting in a ‘reciprocating tachycardia’.
The tachycardia is described as ‘orthodromic’ when conduction within the His bundle is in the normal direction: the ECG then has narrow QRS complexes, and sometimes P waves are visible just after each QRS complex. Less commonly, depolarization passes down the accessory pathway and retrogradely up the His bundle, to cause an ‘antidromic reciprocating tachycardia’, in which the QRS complexes are broad and slurred, and P waves may or may not be seen. When the re-entry tachycardia is associated with a narrow QRS complex (i.e. when it is orthodromic), the pattern resembles a junctional (AV nodal re-entry) tachycardia (see below) and the presence of a preexcitation syndrome may not be suspected ( Figs 3.6 and 3.7).
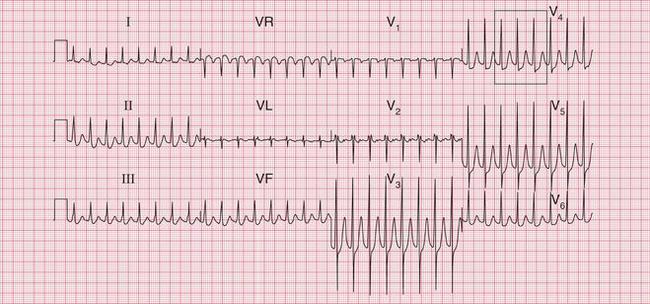

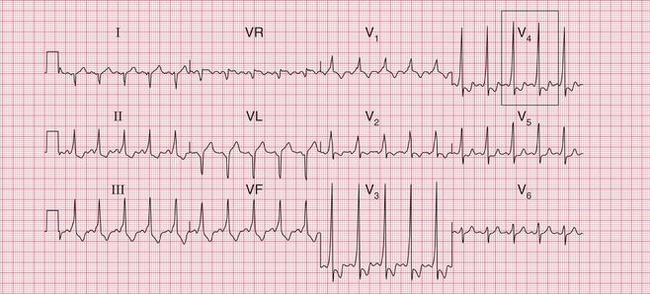

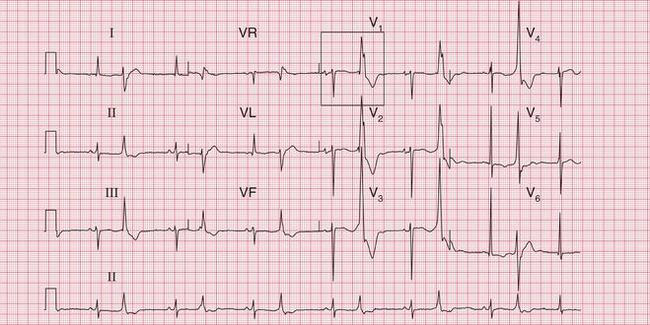
Fig. 3.7 Sinus rhythm, the Wolff–Parkinson–White syndrome, type A
Note
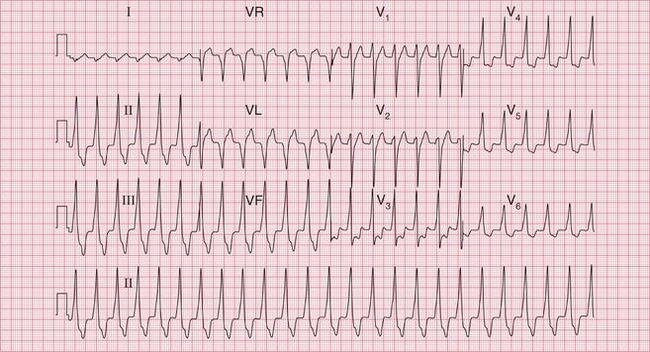
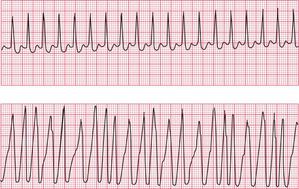
The broad complex (antidromic reciprocating) tachycardias which occur in patients with the WPW syndrome may resemble ventricular tachycardia ( Fig. 3.8). A very irregular broad complex tachycardia, as shown in the lower trace of Figure 3.8, will usually be due to the WPW syndrome with atrial fibrillation and antidromic conduction through the re-entry circuit. This rhythm can only be distinguished with certainty from atrial fibrillation and left bundle branch block if the appearance of the ECG in sinus rhythm is known. Superficially, the rhythm may resemble torsade de pointes ventricular tachycardia, but it lacks the characteristic ‘writhing’ of the QRS complexes that is associated with this arrhythmia.
ATRIAL TACHYCARDIA
Re-entry within the atrial muscle causes a tachycardia characterized by P waves with a shape different from that of those related to sinus rhythm. The PR interval is usually short ( Fig. 3.9). Atrial tachycardia can also result from enhanced automaticity.

ATRIAL FLUTTER
Atrial flutter is an organized atrial rhythm with a rate of 250-350/min. This rhythm depends on a variety of re-entry circuits, which often occupy large areas of the atrium and are known as ‘macro-re-entrant’ circuits. The most common type of flutter, ‘isthmus-dependent’ flutter, involves circuits utilizing the cavotricuspid isthmus. The involvement of a defined isthmus is important in considering ablation therapy (see p. 157).
AV NODAL RE-ENTRY TACHYCARDIA (AVNRT)
Atrioventricular nodal re-entry tachycardia (AVNRT), also known as atrioventricular nodal reciprocating tachycardia, originates in the AV node or His bundle. It may be facilitated by a congenital abnormality of the AV node, in which there are two (or sometimes more) electrically distinct pathways. These allow re-entry to start and be sustained within the node itself. In the absence of a tachycardia, the ECG has no distinguishing features, so the potential for an AVNRT cannot be detected from the ECG, unlike in cases of the WPW and LGL syndromes. During AVNRT, atrial and ventricular activation are virtually simultaneous, so the P wave is hidden within the QRS complex ( Fig. 3.10). AVNRT used to be called ‘junctional tachycardia’.

VENTRICULAR TACHYCARDIA
Ventricular tachycardia may be due to re-entry through circuits within the ventricles (for example around areas of scar tissue following myocardial infarction), or may result from enhanced automaticity or triggered activity. The broad QRS complexes are of a constant configuration and are fairly regular if the re-entry pathway is constant ( Fig. 3.11).

DIFFERENTIATION BETWEEN RE-ENTRY AND ENHANCED AUTOMATICITY
Except in the case of the pre-excitation syndromes, there is no certain way of distinguishing from the surface ECG between a tachycardia due to enhanced automaticity and one due to re-entry. In general, however, tachycardias that follow or are terminated by extrasystoles, and those that can be initiated or inhibited by appropriately timed intracardiac pacing impulses, are likely to be due to re-entry ( Figs 3.12 and 3.13).

TACHYCARDIAS WITH SYMPTOMS
SINUS RHYTHM CAUSING SYMPTOMS
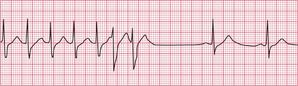
Sinus rhythm can be irregular (sinus arrhythmia) but the patient is never aware of this. The ECG of a patient with sinus arrhythmia ( Fig. 3.14) may suggest atrial extrasystoles – but in sinus rhythm, P wave morphology is constant while with atrial extrasystoles it varies.

Patients often complain of palpitations that are due to sinus tachycardia: the main causes are exercise, anxiety, thyrotoxicosis and the treatment of asthma with beta-adrenergic agonists, and other causes are summarized in Box 1.1 (p. 3). The ECG in Figure 3.15 shows sinus tachycardia due to an unusual cause – the habitual drinking of large quantities of cola.
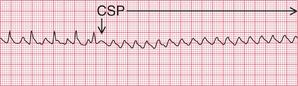
When sinus tachycardia results from anxiety, heart rates of up to 150/min are possible and the rhythm may be mistaken for an atrial tachycardia. Pressure on the carotid sinus will cause transient slowing of the heart rate and the P waves will become more obvious (see Fig. 3.53, p. 153).
EXTRASYSTOLES CAUSING SYMPTOMS
An ECG is necessary to differentiate between supraventricular and ventricular extrasystoles.
When extrasystoles have a supraventricular origin ( Fig. 3.16), the QRS complex is narrow and both it and the T wave have the same configuration as in the sinus beat. Atrial extrasystoles have abnormal P waves. Junctional (AV nodal) extrasystoles either have a P wave very close to the QRS complex (in front of it or behind it) or have no visible P waves.
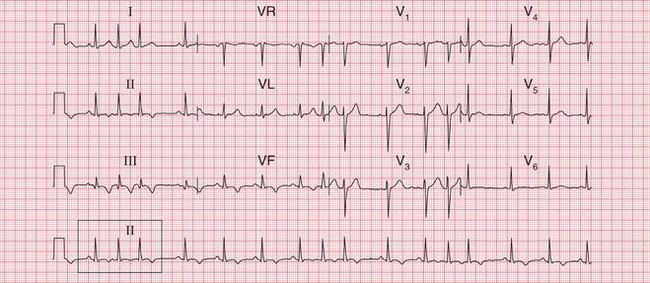

Fig. 3.16 Supraventricular extrasystoles
Note
First beat: normal; second beat: atrial extrasystole, with abnormal P wave; third beat: AV nodal (junctional) extrasystole, with no P wave
Ventricular extrasystoles produce wide QRS complexes of abnormal shape, and the T wave is also usually abnormal. No P waves are present ( Fig. 3.17).

When a ventricular extrasystole appears on the upstroke of the preceding beat, the ‘R on T’ phenomenon is said to be present ( Fig. 3.18). This can initiate ventricular fibrillation, but usually it does not do so.
NARROW COMPLEX TACHYCARDIAS CAUSING SYMPTOMS
A tachycardia can be described as ‘narrow complex’ if the QRS complex is of normal duration, i.e. < 120 ms. Although sinus, atrial and junctional arrhythmias are all supraventricular, the term ‘supraventricular tachycardia’ is often inappropriately used interchangeably with junctional or atrioventricular nodal re-entry tachycardia (AVNRT). All these supraventricular rhythms have QRS complexes of normal shape and width, and the T waves have the same shape as in the sinus beat.
Types of narrow complex tachycardias are listed in Box 3.1.
ATRIAL TACHYCARDIA
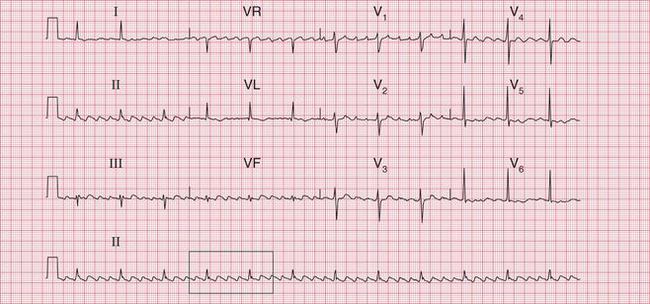
In atrial tachycardia ( Fig. 3.19), P waves are present but they have an abnormal shape. They are sometimes hidden in the T wave of the preceding beat.
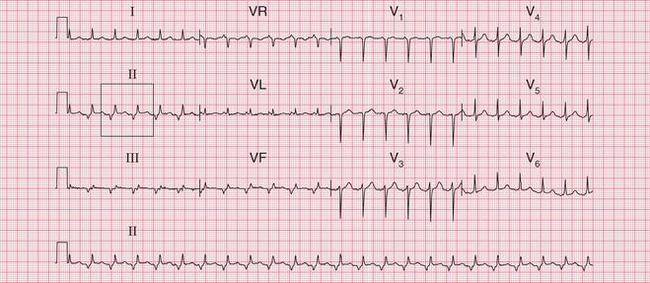

Fig 3.19 Atrial tachycardia
Note
ATRIAL FLUTTER
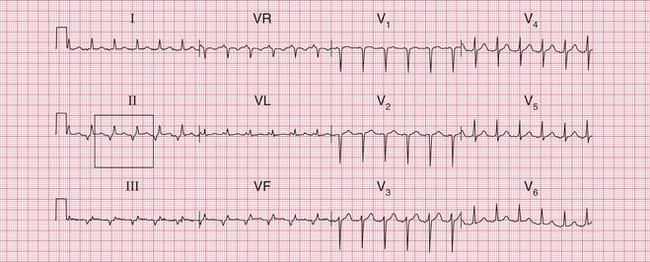
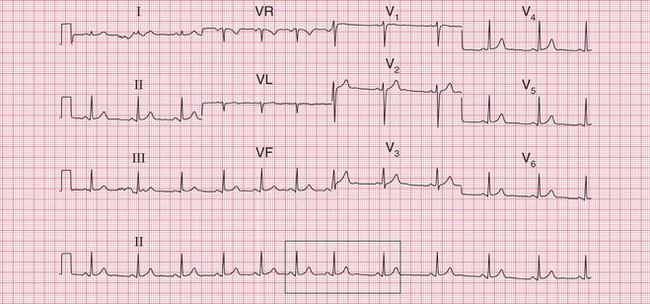
In atrial flutter, the atrial rate is 300/min and the P waves form a continuous ‘sawtooth’ pattern. As the AV node usually fails to conduct all the P waves, the relationship between P waves and QRS complexes is usually 2 : 1, 3 : 1 or 4 : 1. Figure 3.20 shows atrial flutter with 2 : 1 block, giving a ventricular rate of 150/min. The ECG in Figure 3.21 is from the same patient after reversion to sinus rhythm.
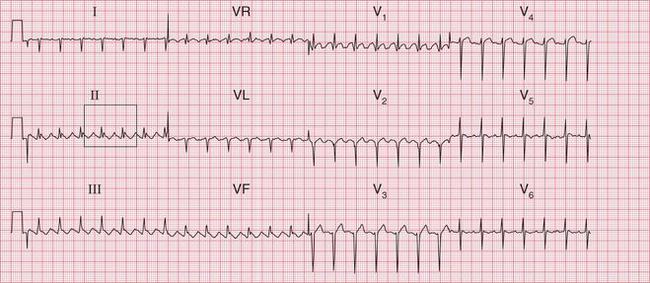

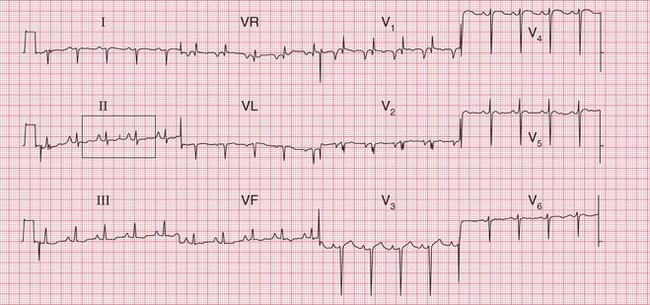
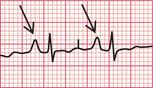
Fig 3.21 Sinus rhythm, following cardioversion
Note
• Same patient as in Figure 3.20
• Deep S waves in lead V6, suggesting right ventricular hypertrophy
• The cardiac axis and QRS complexes have not been changed by cardioversion
The ECG in Figure 3.22 shows atrial flutter with 4 : 1 block.

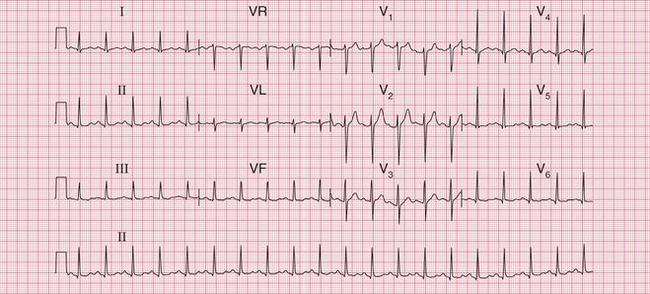
The ECG in Figure 3.23 shows a narrow complex (and therefore supraventricular) rhythm with a rate of 300/min. This is almost certainly atrial flutter with 1 : 1 conduction.
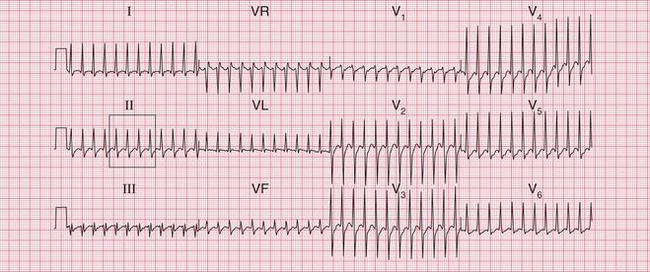

Fig 3.23 Atrial flutter with 1:1 conduction
Note
• Narrow complex tachycardia at nearly 300/min
• Ventricular rate suggests that the underlying rhythm is atrial flutter
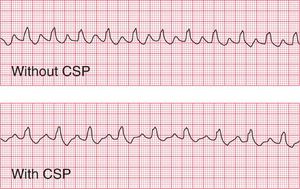
If the ventricular rate is rapid and P waves cannot be seen, carotid sinus pressure will usually increase the block in the AV node and make the ‘sawtooth’ more obvious (see Fig. 3.54, p. 153).
ATRIOVENTRICULAR NODAL RE-ENTRY TACHYCARDIA (AVNRT) OR ‘JUNCTIONAL’ TACHYCARDIA
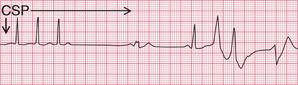
In AVNRT, no P waves can be seen ( Fig. 3.10, p. 110). Carotid sinus pressure either reverts the heart to sinus rhythm or has no effect (see Fig. 3.55, p. 153).
The ECG in Figure 3.24 shows a narrow complex tachycardia at 150/min, without any obvious P waves. After reversion to sinus rhythm ( Fig. 3.25), the shape of the QRS complexes does not change.
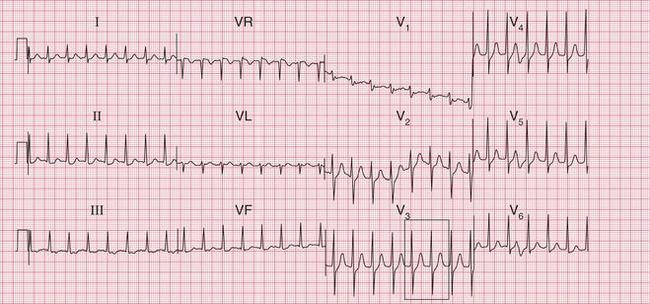

Fig 3.24 Atrioventricular nodal re-entry tachycardia (AVNRT)
Note
• Regular narrow complex tachycardia, rate 150/min
• ST segment depression in leads II–III, VF suggests ischaemia
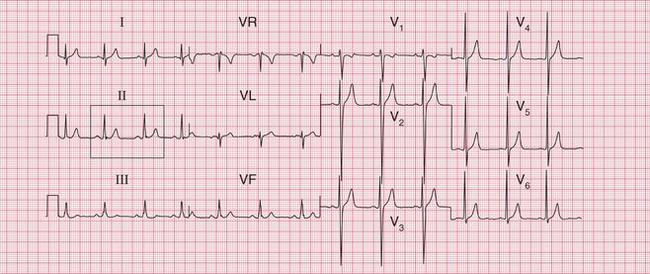

Fig 3.25 Sinus rhythm following cardioversion
Note
• Same patient as in Figure 3.24
• QRS complexes and T waves are the same shape as in AVNRT ( Fig. 3.24)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


