4
The ECG When the Patient has a Bradycardia
MECHANISM OF BRADYCARDIAS
The causes of sinus bradycardia have been discussed in Chapter 1 (see Box 1.2, p. 5). Escape rhythms have been discussed in Chapter 2 (p. 82 ) . They are usually asymptomatic, but symptoms occur when the automaticity that generates the escape rhythm is inadequate to maintain a cardiac output. A bradycardia may cause the symptom of syncope; some of the possible underlying causes are listed in Box 4.1.
SINOATRIAL DISEASE – THE ‘SICK SINUS SYNDROME’
Disordered SA node function can be familial or congenital and can occur in ischaemic, rheumatic, hypertensive or infiltrative cardiac disease. It is, however, frequently idiopathic. Abnormal function of the SA node may be associated with failure of the conduction system. Many patients with sinoatrial disease are asymptomatic, but all the symptoms associated with bradycardias – dizziness, syncope and the symptoms of heart failure – can occur. Atrial and junctional tachycardias often occur together with sinus node dysfunction, when the patient may present with palpitations.
The abnormal rhythms seen in the sick sinus syndrome are listed in Box 4.2.
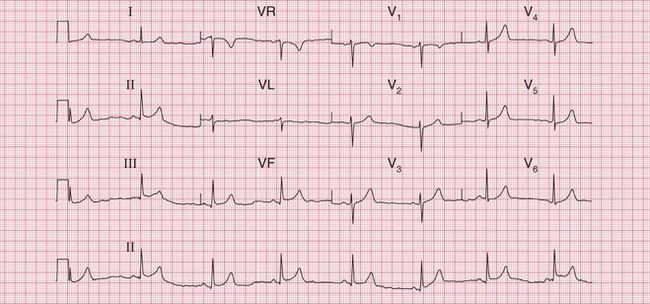
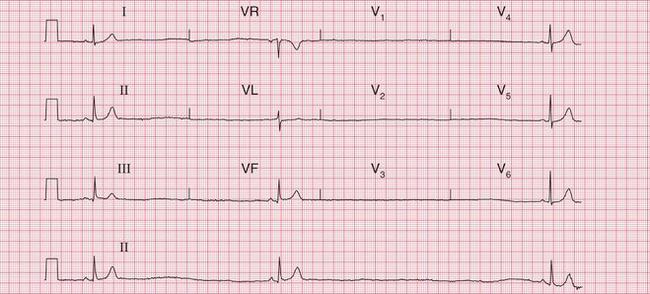
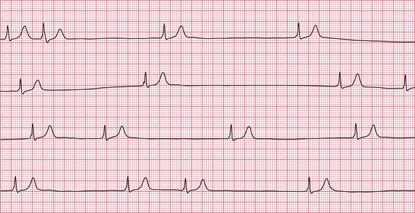
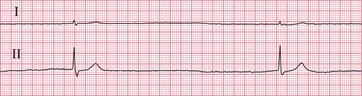
The ECGs in Figures 4.1 and 4.2 are from a young man who had a normal ECG with a slow sinus rate when asymptomatic, but intermittently became extremely dizzy when he developed a profound sinus bradycardia.
The ECG in Figure 4.3 shows an ambulatory record from a young woman who complained of short-lived attacks of dizziness. When she had these, the ECG showed sinus pauses.
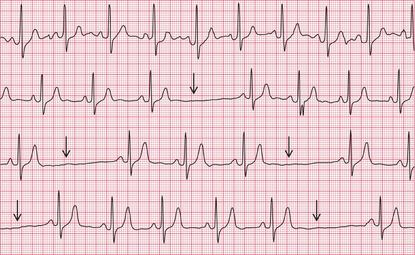
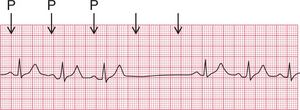
Figure 4.4 shows the other variety of sinus pause – sinus arrest.
The ECG in Figure 4.5 shows an example of a ‘silent atrium’, when the heart rhythm depends on the irregular depolarization of a focus in the AV node.
The combination of sick sinus syndrome and episodes of tachycardia is sometimes called the ‘bradycar- dia-tachycardia syndrome’ and Figure 4.6 shows the rhythm of a patient with this syndrome. This patient was asymptomatic at times, when his ECG showed a ‘silent atrium’ with a slow and irregular junctional (AV nodal) escape rhythm, but he complained of palpitations when he had an AV nodal tachycardia.
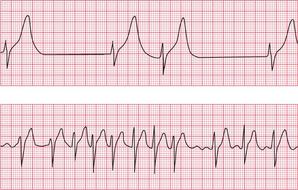
Figure 4.7 shows the ECG from a patient who, when asymptomatic, showed first degree block and right bundle branch block. He complained of fainting attacks, and an ambulatory recording showed that this was due to sinus arrest with a very slow AV nodal escape rhythm, giving a ventricular rate of 15/min ( Fig. 4.8, p. 177). This is an example of the combination of conduction system disease and sick sinus syndrome.
Possible causes of sick sinus syndrome are listed in Box 4.3.
ATRIAL FIBRILLATION AND FLUTTER
A slow ventricular rate can accompany atrial flutter or atrial fibrillation because of slow conduction through the AV node and His bundle systems ( Figs 4.9 and 4.10). This may be the result of treatment with drugs that delay AV nodal conduction, such as digoxin, beta- blockers or verapamil, but can occur because of conducting tissue disease.
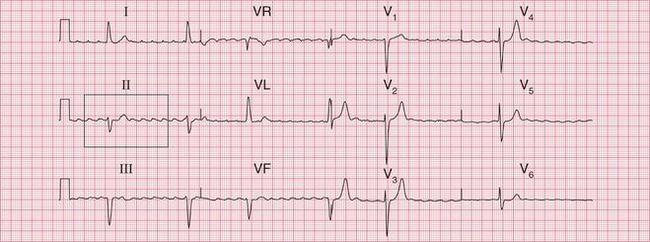

Fig. 4.9 Atrial flutter with variable block
Note
• Flutter waves at 300/min obvious in all leads
• Ventricular rate varies, range 30–55/min
• QRS complex duration slightly prolonged (128 ms), indicating partial right bundle branch block
• There is not complete block, as shown by the irregular QRS complexes


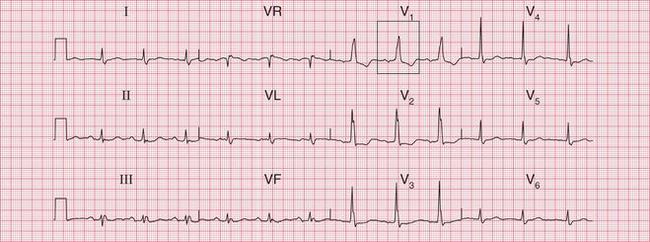
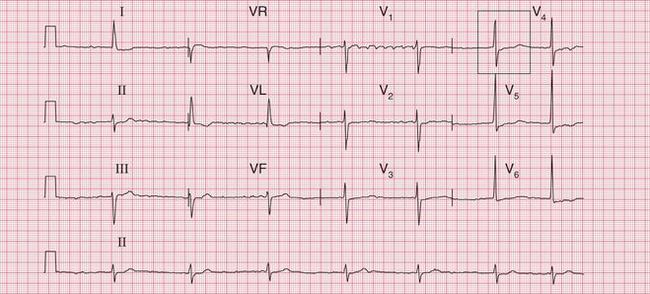
Fig. 4.10 Atrial fibrillation
Note
• Irregular rhythm, rate 43/min
• Flutter-like waves in lead V1 but these are not constant
• QRS complexes otherwise normal
Complete block associated with atrial fibrillation is recognized from the regular and wide QRS complexes which originate in the ventricular muscle ( Fig. 4.11).
ATRIOVENTRICULAR BLOCK
Symptoms are not caused by first degree block, second degree block of the Wenckebach or Mobitz type 2 varieties, left anterior hemiblock or the bundle branch blocks.
Second degree block of the 2:1 or 3:1 type will cause dizziness and breathlessness if the ventricular rate is slow enough ( Fig. 4.12). Young people tolerate slow hearts better than old people do.
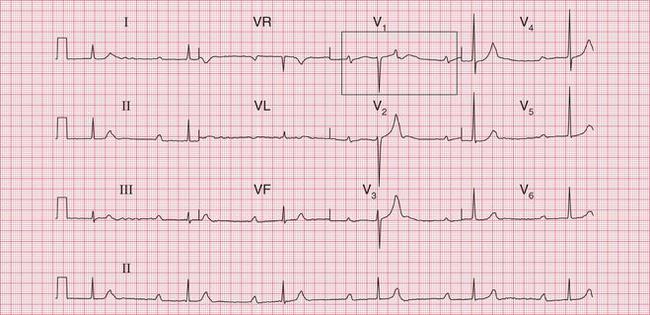

Fig. 4.12 Second degree block (2:1)
Note
• Second degree block, 2:1 type
• Long PR interval in the conducted beats (not characteristic of second degree block)
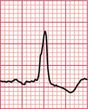
Complete (third degree) block characteristically involves a slow rate, but this may be fast enough to cause only tiredness or the symptoms of heart failure. Figure 4.13 shows the ECG of a 60-year-old man who, despite a heart rate of 40/min, had few complaints.
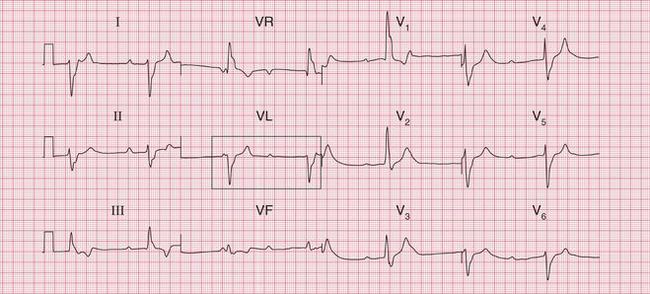
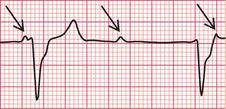
Fig. 4.13 Complete heart block
Note
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


