The Cost Effectiveness of Cardiac Resynchronization Therapy
The Cost Effectiveness of Cardiac Resynchronization Therapy
Dhruv S. Kazi
Mark A. Hlatky
Heart failure is a significant public health problem in the United States, with roughly 5 million Americans living with it. Despite improved understanding of its pathophysiology, heart failure remains a major cause of morbidity and mortality, and is currently responsible for at least 20% of all hospital admissions among persons older than 65.1 Cardiac resynchronization therapy (CRT) represents a new therapeutic approach to the management of heart failure, and has been shown in randomized clinical trials to reduce symptoms, heart failure hospitalizations, and heart failure deaths.1,2,3,4,5,6,7,8,9 The effect of this novel but expensive therapy on total cost of care is an important consideration as the prevalence of heart failure—and the use of CRT—increases in the general population. We summarize the data on the economic outcomes of CRT and discuss its cost-effectiveness.
CONTEXT
Because health care resources are limited, economic principles can be applied to assess how to use these resources most efficiently. Committing resources to a particular use implies that they are no longer available for other uses. This is the concept of opportunity cost—the true cost of utilizing resources is the cost of not being able to put them to their best alternative use.
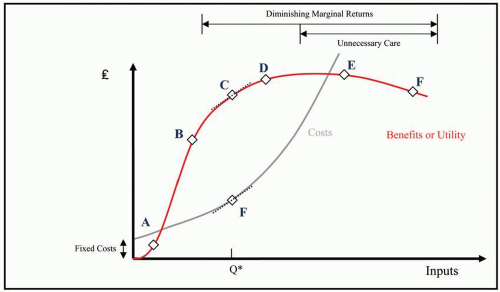
A second key economic principle is the law of diminishing marginal returns (Fig. 13.1), which says that the benefit obtained from providing an additional unit of goods or services decreases progressively with the quantity of resources used. As shown in Figure 13.1, the optimal point for the system to operate is when marginal benefit equals marginal cost. In the medical context, care is considered to be cost-effective when the value obtained from additional expenditures remains “reasonable”—at point C rather than point D in Figure 13.1.
While the development of new diagnostic and therapeutic technologies forms the basis of modern medical progress, it is also a major driving force behind the rapid increase in health care costs. Historically, the approval of new medical technology has required only the demonstration of safety and efficacy. However, as governments struggle to rein in health care expenses, the additional benchmark of cost-effectiveness has been added in many countries, either as a requirement for approval (in Australia and Ontario, Canada, for example) or for adoption by the health care system (in England). Demonstration of cost-effectiveness is not, however, required in the United States. Proponents of considering cost-effectiveness argue that, if a new technology is to be adopted, it should demonstrate not only superiority in safety or efficacy compared with available therapeutic options, but also that it adds value for the patient (or the health care system or society) commensurate with its additional cost.
The value of a new technology like CRT can be gauged by comparing it with an existing therapeutic alternative (optimal pharmacologic therapy, OPT), and calculating the incremental cost-effectiveness ratio (ICER). The numerator of the ICER is the total net cost of using the new therapy compared with using the alternative therapy, and the denominator of the ICER is the total net effectiveness of using the new therapy compared with using the alternative therapy:
Incremental Cost Effectiveness Ratio (ICER)
Three key concepts emerge from the above equation.
First, the choice of comparators is paramount when assessing a new technology. For instance, consider two new technologies, cardiac resynchronization without and with defibrillation capability (CRT-P and CRT-D, respectively). The CRT-D device is almost three times as expensive as the CRT-P device, and has a shorter battery life, thereby incurring higher initial as well as long-term costs. While performing a health care economic evaluation, should both these new technologies be compared with optimal pharmacologic therapy, or should the most expensive technology be compared with the second most expensive technology? A prudent purchaser would first compare CRT-P with OPT, and then compare CRT-D with CRT-P to judge whether the significant cost of adding the defibrillation capability is justifiable.10 Cost-effectiveness is a relative measure, not an absolute measure; a therapy can only be “cost-effective” compared with an alternative (Table 13.1).
FIG. 13.1. The Law of Diminishing Marginal Returns in Health Care. As increasing amounts of inputs are committed to health care, costs (grey curve) rise progressively. The benefits (red curve), on the other hand, do not. Moving from A to B and from B to C requires an equal increase in inputs, but the benefits gained from moving from B to C are substantially lower. Moving from E to F is actually harmful—in health care, as in life, more is not always better. The optimal point for the system to operate is where the cost of producing one additional unit of the goods or services (the marginal cost) is equal to the benefit obtained from producing that additional unit (marginal benefit), at point Q*.
Second, the ICER is based on assessing the complete costs and the complete benefits of each treatment, not merely their initial costs and short-term outcomes. Cardiac resynchronization has a significant upfront cost (of device implantation), so evaluating its cost-effectiveness over a short time-horizon, say of one or two years, may not provide a complete and balanced picture of its value in patient care. In particular, the high initial costs related to implanting the device may be offset over time by reducing hospitalizations, including costly admissions to the intensive care unit. The need for regular interrogations and periodic battery replacements, and the potential for device-related complications, however, could increase overall costs of device therapy. Thus a long-term perspective is essential to obtain a complete picture of costs and benefits of CRT. While measuring costs and effects over the lifetime of the patient would be ideal, the key is that the follow-up in the analysis be sufficiently long to capture all of the relevant costs and benefits, and thereby provide an unbiased assessment of the costeffectiveness of the device.
TABLE 13.1 The Choice of Comparator
Therapy
Cost ($)
Effectiveness (QALY)
ICER – Relative to OPT ($/QALY)
ICER – Relative to CRT-P ($/QALY)
OPT
46,000
2.3
–
–
CRT-P
59,900
3.01
19,600
–
CRT-D
82,200
3.15
43,000
160,000
A decision analytic model based on data from the COMPANION trial produced the above costs and effects over a 7-year period. The ICER of CRT-P relative to OPT ($19,600/QALY) shows that it is a cost-effective intervention.15 If CRT-D were to be compared with OPT, an ICER of $43,000/QALY would also make it appear cost-effective. However, the appropriate comparator for CRT-D is CRT-P—the next-best alternative—and not OPT. When CRT-D is compared to CRT-P, the ICER rises to $160,000/QALY, which is well above the accepted range of $50,000-75,000/QALY. This example highlights the salience of the appropriate comparator in all cost-effectiveness analyses.
The ICER is usually expressed as dollars per life-year added, which then should be compared to a benchmark in order to interpret the result. Several countries (such as the United Kingdom and the Netherlands) have determined a monetary threshold above which a new technology is no longer considered cost-effective. Although there is no hard and fast threshold for cost-effectiveness in the US, most analysts consider $50,000 to $75,000 per quality-adjusted life year (QALY) to be acceptable, but not cost-effectiveness ratios that exceed $100,000/QALY. These are only rough guides, however, as there is no formal national framework in the United States for systematic health care economic evaluation.
COSTS
The cost of CRT includes the cost of the device and its initial implantation, as well as the costs added by subsequent complications, regular interrogations, and generator replacements, and the costs associated with routine heart failure care, including medications, clinic visits, and hospitalizations. The substantial upfront costs of the device and its implantation may be offset over time by the costs associated with care saved by improved heart failure symptoms. While patients who live longer and have a better quality of life may be able to stay in the labor force and contribute to the economy, these indirect costs associated with changes in productivity are usually omitted from cost-effectiveness studies because they would systematically undervalue treatments for patients who are not working. Home health care is included as a direct medical cost, so a therapy that increases the number of patients who can care for themselves may produce substantial savings. These various costs are borne by different parties but it is best to evaluate the total cost of a new technology from the societal perspective—to consider all medical costs irrespective of who bears them (hospital, patient, or a third-party payer).
EFFECTIVENESS
The clinical effectiveness used in the denominator of the incremental cost-effectiveness ratio is conventionally measured by the extent to which either the quantity or quality of the patient’s life is increased. Quality Adjusted Life Years (QALYs) are preferred as a measure of effectiveness in many analyses because they capture both of these dimensions of improved patient outcomes.11 QALYs are calculated by multiplying the life-expectancy of the patient with a preference weight that reflects the patient’s quality of life on a scale from 0 (death) to 1 (perfect health). For instance, if a patient spends 2 extra years in a health condition associated with preference-weight of 0.3, he would have gained 2 × 0.3 = 0.6 QALYs. The preference weights used to calculate QALYs can be obtained using formal elicitation techniques (e.g., the standard-gamble) or quality of life questionnaires (e.g., Minnesota Living With Heart Failure questionnaire).12
Cardiac resynchronization therapy has been demonstrated in clinical trials to improve functional capacity, symptoms, and quality of life, and to reduce heart failure hospitalizations, and all-cause mortality.9 Given its impact on both quality of life and longevity, the effects of CRT are frequently expressed in the combined unit of QALYs.
COST-EFFECTIVENESS OF CARDIAC RESYNCHRONIZATION THERAPY
The cost and outcomes data used to calculate the ICER may be collected alongside the clinical data while conducting a randomized clinical trial (RCT), which makes individual-level data available for the analysis. As with the clinical data obtained from an RCT, the cost data thus collected may provide an objective measure of the expenses associated with the intervention. However, trial-based assessments of cost-effectiveness have several important limitations. The costs incurred in an RCT may be driven by the study protocol, and are dependent on the characteristics of the patients recruited to the study as well as the clinical centers where the trial is being conducted (which are usually academic centers, and have higher costs). More importantly, RCTs tend to have relatively short durations of follow-up (the longest RCT data available for cardiac resynchronization is less than 3 years of follow-up). These issues may be circumvented by developing a model of the natural history of the disease and the impact of the intervention being studied—which can then incorporate average costs and outcomes from published RCTs or meta-analyses thereof. Moreover, by varying the input parameter, either individually or simultaneously as a group, one can test the robustness of the results provided by the model.
While these arguments make decision-analytic models an attractive approach to health care economic evaluations, these models too have limitations. The most important limitation is that the results of these models are often highly dependent on the assumptions made while developing the model and the choice of input parameters. Thus the underlying assumptions of decision analytic models must always be critically examined, and close attention must be paid to the results of sensitivity analyses.
The cost-effectiveness of CRT has been evaluated by randomized clinical trials as well as by decision analytic modeling.
Randomized Clinical Trial
The Cardiac Resynchronization in Heart Failure (CARE-HF) trial was a randomized clinical trial conducted at 82 clinical centers in 12 European countries.1 A total of 813 patients with New York Heart Association Class III or IV heart failure due to left ventricular systolic dysfunction (LVEF <0.35) and cardiac dyssynchrony were randomized to CRT-P plus medical therapy (n = 409) versus medical therapy alone (n = 404). The cost-effectiveness analysis was specified a priori as a secondary outcome in the protocol and included data from all patients enrolled in the trial.13 Cost of medical care was estimated from the utilization of major medical resources, with costs based on the United Kingdom’s National Health Service reference costs. The cost of the device was assumed to be the mean list price across the devices and countries involved in the trial, and was spread over the potential lifetime of the device accounting for patient survival so that only those costs incurred during the study period were included in the
Only gold members can continue reading. Log In or Register to continue