21
The construction industry
Construction of domestic and commercial structures as well as roads and other public works is performed in virtually all societies. In 2007, 7.8 million workers were employed in the construction sector in the USA, representing 5-6% of total nonfarm employment (source: US Bureau of Labor Statistics, Current Employment Statistics Survey). Occupational health issues, including respiratory disorders, among construction workers are often quite challenging. The great variation in work processes and tasks, as well as the continually changing workplace settings often impede the ability of managers and workers to anticipate, document and prevent hazardous exposures.
The multiplicity of potential respiratory hazards associated with construction jobs guarantees that many physicians will be challenged to manage respiratory diseases among construction workers and to assess the significance of job exposures on disease occurrence in the clinical findings. In this section, we discuss the types of exposures to respiratory hazards that may be encountered in the construction setting and the potential health effects, including (1) nonmalignant conditions; (2) malignancies; and (3) immunologic conditions, with an emphasis on asthma.
21.2 Inhalation hazards in the construction industry
The scope of construction projects ranges from simple, small-scale jobs such as building a deck or patio at a single family home, to massive and complex undertakings such as construction of dams, highways, power plants and office towers. Because of the nature of construction, workers in this industry may experience a diversity of worksite exposures. While a limited number of companies have hundreds or even thousands of employees, construction enterprises are typically small, often employing 75 or fewer individuals, with limited resources to address workplace safety and health. Work settings are frequently nonstandardized and changeable, and to maintain employment, workers often must change jobs and employers as some projects are completed and others are started. On the other hand, there are also large construction companies that can employ several thousand workers. Adjacent construction activities can result in exposures to substances that are unrelated to the worker’s particular job tasks. Considering these factors, as well as the almost daily changes in weather and work locations, the evaluation and control of hazardous airborne exposures for a construction worker are uniquely challenging.
Construction respiratory hazards can be grouped into three main categories: particulates (including fumes), gases and vapors, and sensitizers. This chapter summarizes some of the most commonly recognized hazards in construction work. Exposure to welding fumes can be encountered on construction sites with potential for acute and chronic lung effects, and metal fume fever; however, welding is covered elsewhere in this book (chapter 14) and is not considered further here. Paints are frequently present during construction activities but the health effects of exposure to paints are covered elsewhere (chapter 18). Building materials used in construction are often obtained in the region of the project, to reduce transportation costs of these often bulky and dense materials. The content of masonry, stone and other building materials is thus often determined by the locally available raw materials. To better anticipate potential workplace respiratory hazards, occupational physicians should become familiar with the mineralogy (and particularly the content of free silica and asbestiform fibers) of the materials commonly used for construction in their region. Other exposures often encountered are wood dust and asbestos in removing old pipe fittings in renovations and demolition construction work.
Respirable particles
These include silicates, crystalline silica, fibers, fumes, fungal and mold spores, and wood.
- Silicates – in the construction industry, silicates are often associated with the soil in which the construction activity is taking place. Silicates in the form of clay are commonly encountered during earth works, but may not pose much of a respiratory hazard if they remain damp. Portland cement dust, which may be released during some construction work, is composed largely of calcium silicates, aluminates and alumino-ferrites, but may also contain hexavalent chromium.
- Crystalline silica – the form of crystalline silica most commonly associated with construction is quartz. Quartz is a major component of the earth’s crust and is found in many types of rock, especially sandstone and granite. Respiratory hazard ensues when quartz or other forms of crystalline silica (cristobalite, tridymite) are mechanically disturbed and rendered into respirable-sized particles. Construction sand can be 80-99% quartz, depending on the source. Masonry is generally obtained from natural mineral sources, which also often contain quartz. Mortar for building masonry structures generally consists of silica sand combined with Portland cement and water. Concrete is a mixture of cement, water and appropriately sized mineral aggregate. The aggregate comprises a controlled mixture of sized rock, gravel and sand. The combination of masonry, concrete and steel re-enforcement is prized the world over for its strength, longevity and low maintenance. Hazardous exposures to respirable crystalline silica are possible whenever particulates are generated through disturbance of rock, concrete, mortar or masonry, during new construction, renovation or demolition. Proper engineering controls must be used to prevent dust from becoming airborne.
- Fibers – for occupational health purposes, particles with a length-to-diameter ratio of 3: 1 or greater are considered to be fibers. Respirable fibers are less than 1.3 mm in diameter and can be up to 200 mm long. Fibers may either be man-made (fibrous glass, mineral wool and refractory ceramic fibers) or naturally occurring, such as asbestos. Asbestos is the term used for a special group of naturally occurring silicate minerals. There are several forms of asbestos; the most common is chrysotile, a fibrous form of serpentine. When disturbed, asbestos breaks into respirable filaments. In the USA, Europe and elsewhere, because of restrictions on its use (29CFR 1910.1001 OSHA, 40CFR61 and 40CFR763 EPA, Commission Directive 1999/77/EC), asbestos is generally only encountered in the construction industry during renovations and demolition of industrial and commercial structures in which it was used for thermal insulation. Fibrous glass is used for thermal and acoustic insulation, in the form of flexible blankets or rigid boards, and is also used in bathroom fixtures such as tubs, sinks and shower stalls. Fibrous glass may also be added to particular types of concrete and mortar for its strength and thermal properties. Mineral wools have applications similar to those of fibrous glass. Refractory ceramic fibers are spun from molten kaolin clay, silica and minor amounts of oxides. Because of their thermal insulation properties, refractory ceramic fiber products are used to insulate furnaces, stoves and chimneys, and to protect industrial equipment from high temperatures.
- Fumes – fumes encountered in the construction industry include metals from welding/torch cutting, products of combustion including diesel and other fuels, and hot asphalt (see http://www.osha.gov/SLTC/weldingcuttingbrazing/chemicals.xhtml).
- Fungi and molds – contaminated drywall, carpet, wood or other surfaces may be encountered especially during renovation and demolition. Varieties of aspergillus, plasmopara viticola, dictyostelium discoideum, tricoderma koningii, slime molds and other fungi and molds may be present.
- Wood – beech and oak are confirmed human carcinogens. Birch, mahogany, teak and walnut are suspected human carcinogens. A number of commercially important tree species are also known or suspected to induce respiratory sensitization (see Appendix D of 2006 ACGIH TLV, p. 84). Sawing or other contact with wood that has been treated to retard deterioration may result in worker exposures to oxides of chromium, copper and arsenic. Chromated copper arsenate, acid copper chromate, ammoniacal copper arsenate and ammoniacal copper zinc arsenate are or were common compounds used in wood treatment.
Gases
Gaseous exposures during construction work may include oxygen, ozone, oxides of nitrogen and acetylene used in welding and oxy-acetylene cutting of metals.
Chemical vapors
Chemical vapors may be present from evaporation of solvents, paints, laquers, fuels and oils associated with heavy construction equipment or from off-gassing of construction materials such as carpeting and plywood.
Sensitizers and asthmagens
Diisocyanates are important sensitizers often encountered in the construction industry and may be components of adhesives, epoxies, paints and spray thermal insulation. Other sensitizing exposures include chromium and nickel compounds (for welders and cutters); resins (electricians); soldering fumes and welding fumes (welders); wood dust and formaldehyde (construction carpenters); water-based paints with azidine and lacquers with formaldehyde and microbiocides (painters and lacquerers); chromiumcontaining cement dust and epoxy adhesives (bricklayers and tile setters); and methylmethacrylates (reinforced concrete layers). Numerous other man-made and naturally occurring substances are classified as asthmagens (see AOEC website list: http://www.aoec.org/tools.htm).
21.3 Diseases associated with exposures in construction work
21.3.1 Chronic obstructive pulmonary disease and the pneumoconioses
Chronic obstructive pulmonary disease (COPD) is characterized by airflow limitation that is not fully reversible. Predominant pathological features of COPD are emphysema, small airways disease and chronic bronchitis. The association between occupational exposures to dusts, gases and fumes and COPD was firmly established through a series of systematic epidemiological investigations. In 2002, the American Thoracic Society estimated that, based on the available epidemiologic evidence, about 15% of all cases of COPD in the US population were attributable to occupational exposures. Nevertheless, because COPD is also associated with tobacco smoking, which is prevalent among construction workers and other blue collar populations, the role of occupational exposures in the etiology of COPD is often neglected.
Depending on the specific work processes and the effectiveness of dust control activities, construction workers can potentially be exposed to relatively high levels of fibrogenic mineral dusts (e.g. asbestos and silica), causing pneumoconiosis, and non- or weakly-fibrogenic dusts, which can also be associated with adverse lung effects (e.g. emery, graphite, gypsum, marble, mica, plaster of Paris, Portland cement, silicon, soapstone). Other harmful exposures in construction that can increase the risk of chronic airflow limitation include irritant gases and fumes (e.g. welding, painting, blasting fumes, combustion exhaust, asphalt, adhesives, sealants, hydrochloric acid), man-made mineral fibers and organic dust (e.g. wood). Airflow limitation in construction workers may thus be related to mineral dust-induced pneumoconiosis and nonfibrotic changes in airways associated with exposures to dusts, gases and fumes. The effects of each of these agents may be aggravated in some exposed individuals by associated mycobacterial lung infections. Although the adverse effects of many of these agents has been established in epidemiologic studies conducted across a wide spectrum of industrial workers, epidemiologic research carried out among construction workers has helped to ascertain the potential of the above agents for causing respiratory mortality and morbidity in these workers.
COPD Mortality Studies
Taken together, studies carried out among construction workers in different countries have shown a clear pattern of elevated respiratory disease mortality, although there is variation in the strength of the association with construction employment; the differences may in part be explained by differing construction techniques, materials, and dust control programs.
In the USA, surveillance data indicate that the number of deaths from asbestosis and silicosis is highest in workers who report they have worked primarily in the construction industry. Asbestosis deaths represented about one-third of all pneumoconiosis mortality during the 10-year period from 1990 to 1999 and the annual number of asbestosis deaths among US residents continues to increase. Occupations with the highest adjusted proportional mortality rate (PMR) from asbestosis are insulation workers, boilermakers, plumbers, pipe-fitters, plasterers, electricians, welders, brick and stone masons, crane and tower machine operators, and carpenters. Reports of deaths from silicosis in the USA declined from 1968 to 1999; in recent years the construction industry has accounted for 13.4% of all deaths from silicosis. Occupations with elevated PMR from silicosis included machine operators and construction labourers.
US surveillance data also demonstrate elevated COPD mortality in the construction industry (Table 21.1). Occupations with elevated mortality included a number of construction trades: excavation and loading machine operators, followed by drywall installers, painters, construction and maintenance, carpenters and construction labourers. Smoking can potentiate the effect of construction exposures on COPD. A mortality study of California construction workers found an elevated adjusted standardized mortality ratio (SMR) for COPD, but SMRs for other unhealthy lifestyle-related causes of death were also significantly elevated.
Table 21.1 Summary of epidemiologic findings: mortality studies among construction workers
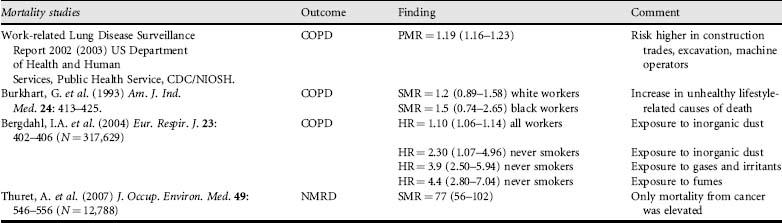
NMRD = non-malignant respiratory disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


