In 2003 a task force cosponsored by the American College of Cardiology, American Heart Association, and American Society of Echocardiography published guidelines for clinical application of echocardiography, including trauma and critical care. The full-text article is available from the Web sites of each organization and the summary is published in the journals of each group (1). As is the case with most such guidelines, they are structured in terms of recommendations according to the level of scientific support, with “Class I” indications defined as “conditions for which there is evidence and/or general agreement that a given procedure or treatment is useful and effective.” Other levels of evidence are “Class IIa” where there is some divergence of opinion but the weight of evidence is in favor of utility/efficacy; “Class IIb” where the weight of evidence is less compelling; and “Class III” where the evidence suggests either a lack of utility or even harm. Table 21.1 lists the conditions relevant to critical care and trauma where the 2003 guidelines suggest Class I indications. In addition, Class I or IIa indications for echocardiography exist for many conditions that may coexist or present in the critically ill (e.g., known or suspected native or prosthetic valve endocarditis; chest pain and/or myocardial ischemic syndromes; dyspnea, edema, or cardiomyopathy; pericardial disease; suspected thoracic aortic disease; and pulmonary/pulmonary vascular disease).
TEE provides a particular benefit in the critically injured and the critically ill. Unlike the echocardiography laboratory where adequate images can be obtained from the transthoracic exam in > 90% of patients (2), the percentage of successful, diagnostic TTE exams in the critically ill is approximately 50% (3,4,5,6,7,8). Several reports of TEE in this population are based entirely on patients in whom TTE could not obtain adequate images (9,10,11,12,13); in all of these reports, the success rate in obtaining an adequate TEE exam was > 90%. Conditions limiting the effectiveness of TTE are listed in Table 21.2. In addition, there are the “usual” indications for preferential use of TEE (high-resolution imaging of structures nearer to the esophagus than the chest wall) in many critically ill or injured patients. It has been suggested that TTE is not cost-effective in critically ill surgical patients and the usual progression of TTE followed by TEE should be replaced by directly performing a TEE exam in this population (14). Most would not agree with this view because TTE is a noninvasive, rapid test, becoming even more available to clinicians with the recent appearance of handheld transthoracic devices (Figs. 21.1 and 21.2). In critically ill and injured patients these smaller, portable devices suffer the same drawbacks as listed in Table 21.2, and are not currently able to provide the full echocardiography examination, but they are small, simple, and convenient to use and can facilitate an urgent, focused, qualitative assessment in many patients (10). The fact remains, however, that definitive diagnosis for approximately 50% of critically ill or injured patients will require a TEE exam.
TABLE 21.1. Class I Indications for Echocardiography in the Critically Ill and Critically Injured (1)
Critically Ill
1.
The hemodynamically unstable patient
2.
Suspected aortic dissection (TEE)
Critically Injured
1.
Serious blunt or penetrating chest trauma (suspected pericardial effusion or tamponade)
2.
Mechanically ventilated multiple-trauma or chest trauma patient
3.
Suspected preexisting valvular or myocardial disease in the trauma patient
4.
The hemodynamically unstable multiple-injury patient without obvious chest trauma but with a mechanism of injury suggesting potential cardiac or aortic injury (deceleration or crush)
5.
Widening of the mediastinum, postinjury suspected aortic injury (TEE)
6.
Potential catheter, guidewire, pacer electrode, or pericardiocentesis needle injury with or without signs of tamponade.
FIGURE 21.1. Handheld ultrasound unit made by Sonosite, Inc. (Vascular access probe is shown; a 2 MHz cardiac probe is available.)
In this chapter the use of echocardiography to assess the hemodynamically unstable patient in the intensive care unit (ICU) or emergency room (ER) will be discussed, followed by evaluation of the patient with unexplained hypoxemia (question of intracardiac shunt), and the patient with suspected endocarditis. Finally the assessment of the patient with trauma, and with suspected aortic dissection will be presented. Table 21.3 lists these and other common indications for echocardiography in the ICU.
FIGURE 21.2. Handheld ultrasound unit made by Philips Inc.
TABLE 21.2. Conditions Limiting Success of Transthoracic Imaging in the ICU
Mechanical ventilation
Especially PEEP > 15 cm H2O
Inaccessible windows
Surgical dressings and drains
Chest tubes
Thoracic or upper abdominal incisions
Pneumothorax, pneumopericardium, or subcutaneous emphysema
Surgery-induced fluid collections or cardiac position changes
Inability to position patient
Inability of patient to cooperate for respiratory maneuvers
Obesity
Severe chronic obstructive pulmonary disease
The Hemodynamically Unstable Patient
“Hemodynamic instability” usually refers to unexplained hypotension or hypotension not responding appropriately to fluid or vasopressor therapy. This is a common clinical problem in the ER and ICU. Some conditions associated with hypotension and the associated echocardiographic findings are indicated in Table 21.4. Heidenreich et al. studied 60 patients with unexplained hypotension, finding adequate images with TTE in 36%, but in 97% with TEE (4). He reported new diagnoses in 28%, leading to surgery in 20%. Sohn et al. (11) performed 127 examinations over 7 years, and found “severe cardiovascular abnormalities” accounting for unstable hemodynamics in 52%, with 21% undergoing urgent procedures based on the TEE findings. Several other reports suggest significant changes in therapy or surgical intervention following TEE examination in many ICU populations including those with hypotension (5,8,11,12). In addition to imaging specific pathologies that may indicate a need for surgical repair or intervention, assessment of ventricular size and contractility in combination with diastolic properties permits differentiation between cardiac and noncardiac causes of hypotension. Not surprisingly, TEE is of particular value after cardiac surgery, when mechanical ventilation, incisional dressings, and chest tubes are always present. Three reports in this population demonstrate how TEE may prompt additional surgery and prevent unnecessary reoperation in the postoperative cardiac patient (15,16,17). Denault et al. elegantly describe the value of repeat TEE examination after lung transplantation, providing not only diagnostic information, but also the placement of the intraaortic balloon pump, cannulae for extracorporeal membrane oxygenation, and weaning from the latter therapy were all facilitated by use of TEE (18).
TABLE 21.3. Common Reasons for Requesting Echocardiography in the ICU and ER
Hypotension with lack of response to fluid administration
Assessment of intravascular volume status
Assessment of myocardial function: left and right
Known or suspected chest trauma
Suspected aortic dissection
Suspicion of pulmonary embolus (right heart function; look for clot)
Suspicion of new valvular disease (e.g., mitral regurgitation)
Prosthetic valve dysfunction
Suspicion of endocarditis
Suspicion of pericardial disease (e.g., tamponade)
Hypoxemia with suspicion of intracardiac shunt
Chest pain
Complications of myocardial infarction
TABLE 21.4. Some Common Conditions Associated with Hypotension
Condition
Useful Views
TEE Findings
Hypovolemia
TG SAX of LV
Decreased EDA
TG LAX of LV
Increased FAC “Kissing” papillary muscles
Vasodilation
TG SAX of LV
Normal EDA Increased FAC
ME 4 Ch, 2 Ch, LAX
No severe valvular regurgitation
Decreased
TG SAX of LV
Increased EDA, decreased FAC
Systolic
TG LAX of LV
Increased ESA, decreased FAC
Function
Pericardial Tamponade
ME 4 ch; TG SAX and LAX of LV
Effusion Diastolic collapse of right-sided chamber/chambers
Aortic Dissection
ME 5 ch and LAX; ascending/descending Ao
Intimal flap Two lumens in aorta (no flow in 1) Aortic regurgitation Pericardial effusion
Pulmonary Embolus
ME 4 ch; RV in/out; PA views (upper E)
Dilated RA and RV Small LA and LV TR/PR jets Flow through PFO Echogenic density
Modified from Lobato EB, Urdaneta F. “TEE in the ICU” in A practical approach to TEE. Perrino AC, Reeves ST eds. Philadelphia: Lippincott Williams & Wilkins 2003;272-85, with permission.
Echocardiography versus the Pulmonary Artery Catheter
Most of the information available from the pulmonary artery catheter (PAC) can also be obtained from echocardiography. The principal drawbacks to the latter are that it requires significant training and expertise that is not widely available in the ER and ICU, and echocardiography usually provides only a single, diagnostic examination. Invasive monitoring skills are more widespread, and the PAC is used to guide or monitor therapy in a way that would be impractical for echocardiography (although the use of handheld devices as referred to above, and increased echocardiography training for ER and ICU physicians may change this). On the other hand, provided an echocardiographer is available, echocardiography can provide diagnostic information faster than the time required to place and obtain information from a PAC (19), and imaging provides a diagnostic capacity not available from the PAC.
A number of investigators have examined the role of echocardiography when a PAC is already present. In the study by Heidenreich referred to above, a PAC was present in 38% of the patients; 63% had changes in therapy after TEE (4). After cardiac surgery, Reichert et al. found a disagreement in diagnosis in 50% of patients when TEE and PAC were compared (15). Costachescu et al. found TEE was associated with a higher interobserver reliability in the assessment of hemodynamic instability after cardiac surgery than hemodynamic monitoring (17). In a medical-surgical population excluding postcardiac surgery patients, Poelaert et al. found 44% of patients who had a PAC in place had therapy changed after TEE, whether the primary illness was cardiac or septic (20). In an attempt to understand this discrepancy, Bouchard et al. compared ventricular performance assessments from the PAC (left ventricular stroke work index, or LVSWI) with fractional area change (FAC) and regional wall motion score index from TEE in 60 patients during and after cardiac surgery (21). They found no correlation between LVSWI and FAC, and postulate that changes in ventricular compliance, loading conditions, and ventricular function alter the pressure-volume relationship of the left ventricle in a manner that leads to discordant interpretations between the two techniques. This is illustrated in Fig. 21.3 with the use of pressure-volume curves. A simple example would be the effect of acute preload reduction, which decreases LVSWI, but increases FAC (ejection fraction). The use of both techniques (PAC and TEE) simultaneously to aid clinical decision making has not been assessed in a prospective manner; however, many investigators have suggested that use of pressure parameters alone (from the PAC) can lead to erroneous conclusions regarding ventricular filling and function.
Unexplained Hypoxemia: Intracardiac Shunt
In clinical medicine hypoxemia is caused by three disorders:
1. Hypoventilation
2. Impaired gas exchange (most commonly low ventilation-perfusion ratio, or poor ventilation of perfused alveoli; less commonly diffusion impairment)
3. True shunt
FIGURE 21.3. Pressure-volume relationship with left ventricular (LV) pressure on the y-axis and LV volume on the x-axis. The stroke volume (SV) is end-diastolic volume (EDV) minus endsystolic volume (ESV); the ejection fraction (EF) is equal to SV divided by EDV. Three scenarios are presented to explain discrepancy between changes in LV stroke work (LVSW) and EF. On the left, acute preload reduction was associated with a leftward displacement of the pressure-volume relationship. This results in a reduction of LVSW and an increase in EF. In the middle panel, diastolic dysfunction was associated with an upsloping of the pressure-volume relationship. This results in a reduction in LVSW, but no change in EF. Finally, in the right panel, pure systolic dysfunction was associated with a rightward displacement of the pressure-volume relationship. In this condition, LVSW will be unchanged, but EF will be reduced. Reproduced from Bouchard MJ, et al. Crit Care Med 2004;32: 644-48, with permission.
The latter may be intrapulmonary (e.g., lobar collapse) or intracardiac (e.g., patent foramen ovale or PFO). It is not uncommon for more than one of these disorders to occur simultaneously in the critically ill. When there is true shunt, a decrease in the cardiac output resulting in a decreased mixed venous saturation can further worsen the arterial hypoxemia.
Transesophageal echocardiography is the technique of choice for detection of intracardiac shunt (22). In addition, the TEE exam provides an assessment of overall cardiac function and views of other intrathoracic pathology (pericardial or pleural effusions, collapsed portions of the lung, pulmonary embolus). In those patients with persistent unexplained hypoxemia (i.e., not explained by the chest radiograph), echocardiography should be performed to search for an intracardiac shunt, the most common of which is PFO. While less common, atrial septal defects of all types as well as associated anomalous pulmonary venous drainage can best be detected by TEE (23).
Patent Foramen Ovale
In utero, blood from the placenta bypasses the lungs by crossing from the right atrium (RA) to left atrium (LA) through the foramen ovale, a fenestration in the septum secundum located in the fossa ovalis. The fossa ovalis is bordered by a section of the septum primum, which acts as a one-way flap valve. At birth when LA pressure exceeds RA pressure the flap valve functionally seals, but may not form a permanent closure. A Mayo clinic adult autopsy study demonstrated a 27% incidence of “probepatent” foramen ovale (24). In disease states associated with elevations in the RA pressure, this potential channel can open allowing right-to-left shunting. Some examples in the critical care setting include acute pulmonary embolism, right ventricular infarction, and use of high levels of positive end expiratory pressure (PEEP). Less common circumstances include cardiac tamponade and distortion of mediastinal structures that may occur postpneumonectomy. A review of perioperative implications of PFO was recently published (25).
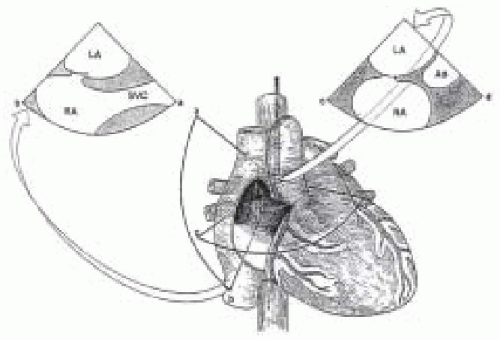
Echocardiographic detection of a PFO and associated intracardiac shunt requires visualization of the atrial septum, color flow mapping, and right-sided injection of echo contrast (contrast echocardiography). Usually the best TEE views of the fossa ovalis are from the midesophageal level; scanning from the horizontal to the vertical plane with the probe rotated to the right will allow a complete assessment, with the best views in the vertical plane (Fig. 21.4). With unenhanced two-dimensional scanning, the size of the fossa ovalis and the mobility of its flap valve can be assessed. The presence of an atrial septal aneurysm, defined as a transient bulging of the fossa ovalis region of the interatrial septum greater than 15 mm in the absence of chronically elevated atrial pressures, is associated with up to a 90% incidence of PFO (26).
FIGURE 21.4. Schematic drawing demonstrating anatomy of interatrial septum as viewed from the right atrial perspective. The potential superiority of the vertical plane (sector image to the left) to delineate opening of the PFO (black shadow in the cranial portion of the fossa ovalis) is related to its craniocaudal orientation. A horizontal cut (sector image to the right) is less likely to intersect the potential separation between the septum primum and septum secundum. The transducer is situated behind the LA. LA, left atrium; RA, right atrium; SVC, superior vena cava; Ao, aorta. Reproduced from Chenzbraun A, et al. J Am Soc Echocardiogr 1993;6:417-21, with permission.
Detection of flow across a PFO requires color flow mapping and contrast echocardiography. Color flow mapping of this region using a low Nyquist limit (30 cm/sec) may detect shunt in either (or both) direction(s). The pressure gradient between the RA and LA can be transiently augmented in an intubated patient by releasing a sustained positive intrathoracic pressure (20 cm water for a few cardiac cycles), or in a spontaneously breathing patient by release of a Valsalva maneuver. The increase in right-sided venous return provoked by this maneuver should cause the interatrial septum to “bulge” to the left, and result in visible flow across the foramen ovale if it is patent. If flow through a PFO is causing hypoxemia, this maneuver should not really be necessary.
Contrast Echocardiography
The definitive test for presence of a PFO is contrast echocardiography, performed by injecting agitated, microbubble-containing solution rapidly into the RA (27). This test does not require actual imaging of the PFO or flow, both of which may sometimes be difficult—especially with TTE. Approximately 5 ml of saline, 3 ml of the patient’s blood, and 0.2 ml-2.0 ml of air are rapidly injected between two 10-ml syringes connected to a stopcock, until the solution is opaque but with no large visible air bubbles. While imaging both atria (Fig. 21.4), the 10-ml solution is rapidly injected into a venous catheter as close to the RA as possible, resulting in “opacification” (made white with microbubbles) of the RA. A right-to-left shunt is diagnosed if microbubbles appear in the LA within three to five cardiac cycles of RA opacification; late appearance can be due to transpulmonary flow. Crude quantification is possible with a small shunt defined as 3-10 bubbles, a medium shunt 10-20, and a large shunt > 20 bubbles (28). If the right-to-left shunt is causing arterial hypoxemia, the contrast test will be positive.
Suspected Endocarditis
Infective endocarditis (IE) may present as critical illness (cardiac failure, dysrhythmias, sepsis), and critically ill patients may develop endocarditis due to infection of indwelling devices and the presence of an immunocompromised state. Because critically ill patients often have nonspecific signs and symptoms, and are usually receiving antibiotics that reduce the sensitivity of blood cultures, echocardiography plays a critical role in diagnosis. A recent review suggests that TEE is cost-effective as an initial strategy (as opposed to TTE) when the pretest (preecho) probability of endocarditis based on clinical findings and laboratory results is as low as 4% (29).
Strict diagnostic criteria for IE were originally proposed by von Reyn et al. in 1981 (30), then revised by Durack et al. in 1994 (the “Duke” criteria) (31). Diagnosis is made based on either (1) pathologic (surgery or autopsy) findings or (2) clinical plus echocardiographic findings. Table 21.5 outlines the clinical criteria defined by Durack et al. They suggest the presence of 2 major criteria, 1 major and 3 minor, or 5 minor criteria all be considered “definite by clinical criteria.” In an evaluation of the Durack criteria in more than 100 patients with IE, Roe et al. found that TEE was critically important, resulting in a diagnostic reclassification in approximately 25% of patients, 90% of which were from “possible” to “definite” IE (32).
The hallmark lesion of IE is the vegetation, defined as a mass adherent to the endocardium consisting of pathologic microorganisms interwoven with platelets, fibrin strands, and blood cells. Vegetations typically occur where normal endocardium has been partially denuded or altered by abnormal flow such as regurgitation, the most common site being the “upstream” side of a regurgitant valve (e.g., the LA side of the mitral valve or LV side of the aortic valve). Vegetations usually occur on valves, but may occur on a chamber wall where the endocardium has been disrupted by abnormal flow, such as a regurgitant jet. Lesions may be relatively slow growing (months) or, in the case of very pathogenic organisms such as staphylococcus aureus, rapidly growing to more than a centimeter in size over a few days. A variable amount of destruction of the involved region of the heart occurs, usually resulting in new or worsening regurgitation; the infection can become invasive leading to localized abscess and/or fistula formation. The echocardiographic appearance is an echodense mass exhibiting a variable amount of independent motion (Fig. 21. 5). Vegetations may vary in size from microscopic (below the resolution of TEE) to several centimeters in size, with fungal vegetations of the tricuspid valve tending to be the largest.
TABLE 21.5. Criteria for the Diagnosis of Infective Endocarditis (IE)
Major Criteria
Positive blood culture
Typical organism for IE from two separate blood cultures* OR Persistently positive blood culture with organism consistent with IE from
(i)
Blood cultures drawn more than 12 hours apart, or
(ii)
All of 3 or a majority of 4 or more separate cultures at least 1 hour apart
Evidence of endocardial involvement
Positive echocardiogram for IE
(i)
Oscillating intracardiac mass on valve or supporting structures, or in the path of regurgitant jets, or on implanted material, in the absence of an alternative anatomic explanation
(ii)
Abscess
(iii)
New partial dehiscence of prosthetic valve, or new valvular regurgitation (change in murmur not sufficient)
Minor Criteria
Predisposition: predisposing heart condition or intravenous drug use
Microbiologic evidence: positive blood culture but not meeting major criteria**
Echocardiogram: consistent with endocarditis but not meeting major criteria
* Viridans streptococci, Streptococcus bovis, HACEK group (Haemophilus spp., Actinobacillus actinomycetemconitans, Cardiobacterium hominis, Eikenella spp., and Kingella kingae); or communityacquired staphylococcus aureus or enterococci, in the absence of a primary focus.
** Excluding single-positive culture for coagulase negative staphylococci and organisms that do not cause endocarditis or serologic evidence of active infection with appropriate organism (31).
Vegetation Detection by TTE versus TEE
Similar to the discussion above regarding the assessment of hemodynamic instability in the ICU, at least 6 investigations in the last 15 years have compared TTE with TEE in the diagnosis of IE. These studies have been summarized by Shanewise and Martin (33), demonstrating a sensitivity of TTE of 28%-63% versus 86%-100% with TEE. The specificity of the two techniques is similar: once a vegetation is seen with either TTE or TEE it is generally due to IE, however TEE provides a much greater sensitivity and is the technique of choice. The less invasive TTE is likely to be performed first in most cases, however, if negative the TTE should be promptly followed by TEE. Several of the studies also found TEE to be much more sensitive in the detection of associated pathology, such as chordal rupture, valve perforation, and abscess formation. All used single-plane TEE; a recent study by Reynolds et al. in 114 cases of suspected IE confirmed that with the use of modern equipment TTE still detects only 55% of lesions seen with TEE (34).
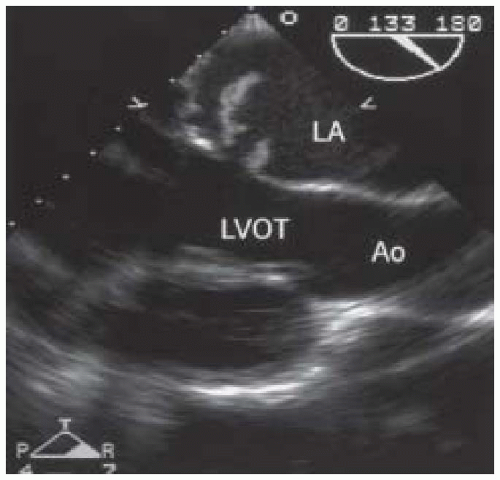
FIGURE 21.5. Midesophageal long-axis TEE view showing a large vegetation on the mitral valve with perforation through the anterior leaflet. LA, left atrium; LVOT, left ventricular outflow tract; Ao, ascending aorta.
The echocardiographic exam for IE should be a complete, standard exam including careful, multiplane imaging of all the valves and associated structures, as well as complete Doppler echocardiographic assessment. In some patients (especially those with prosthetic valves), it may be necessary to use TTE and TEE to obtain adequate views. Care must be taken to evaluate the tissues surrounding any valves with suspicious findings, looking for fistulae and abscesses. Echocardiography can also be used to assess prognosis in IE, because vegetation size and mobility are predictive of outcome (greater size and mobility, worse outcome). One study found that vegetations larger than 10 mm were associated with a 47% risk of embolization (35); another found that 25% of mitral vegetations versus 10% of aortic vegetations were associated with embolization (36). In all series, embolization is a major risk factor for adverse outcome. Thus, large mobile vegetations of the mitral valve are likely to be associated with a poor prognosis.
Trauma
Chest trauma alone accounts for 25% of fatalities from automobile accidents. Due to its noninvasive nature, transthoracic echocardiography (TTE) is initially used as a screening tool for evaluating patients with significant chest trauma. However, as described above there are multiple technical limitations with TTE. Transesophageal echocardiography provides consistently superior resolution of multiple cardiac structures in the setting of trauma, and is especially useful in assessing the thoracic aorta, mitral valve, and posterior structures, such as the left atrial appendage, the intraatrial septum, and the pulmonary veins (37,38,39,40).
In a prospective multicenter trial, Garcia-Fernandez has demonstrated the utility of TEE in the assessment of patients with blunt chest trauma and compared TEE findings with those provided by the electrocardiogram and cardiac isoenzyme assays (40). As outlined in Table 21.6, Garcia-Fernandez demonstrated that 56% of patients had pathologic findings on TEE attributed to blunt chest trauma (Fig. 21.6).
Only gold members can continue reading. Log In or Register to continue