Tachycardias of supraventricular origin sometimes result in broad ventricular complexes. Thus they may mimic ventricular tachycardia. Now that this is widely appreciated, the tendency is to misinterpret ventricular tachycardia as supraventricular, rather than the reverse.
Causes of a broad complex tachycardia
Tachycardias with broad ventricular complexes may be due to:
A number of guides are used to distinguish a supraventricular tachycardia with broad ventricular complexes from ventricular tachycardia.
Useless guidelines
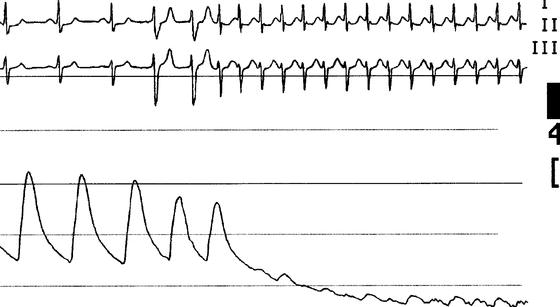
It is often said that whereas ventricular tachycardia leads to major haemodynamic disturbance, supraventricular tachycardia does not. This is wrong. Sometimes ventricular tachycardia causes few or even no symptoms, whereas supraventricular tachycardia, if very fast or in the presence of underlying heart disease, can cause shock or heart failure (Figure 14.1).
Another widely quoted but incorrect rule is that whereas supraventricular tachycardia is regular, ventricular tachycardia is slightly irregular.
Verapamil may terminate supraventricular tachycardia or slow the ventricular response to atrial fibrillation or flutter. It has been used as a ‘therapeutic’ test of the origin of tachycardia. However, dangerous hypotension may result when the drug is given during ventricular tachycardia. Never use verapamil to establish the origin of a broad complex tachycardia.
Useful guidelines
Independent atrial activity
If there is direct or indirect (Figures 12.2, 12.4, 12.10, 14.2, 14.3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


