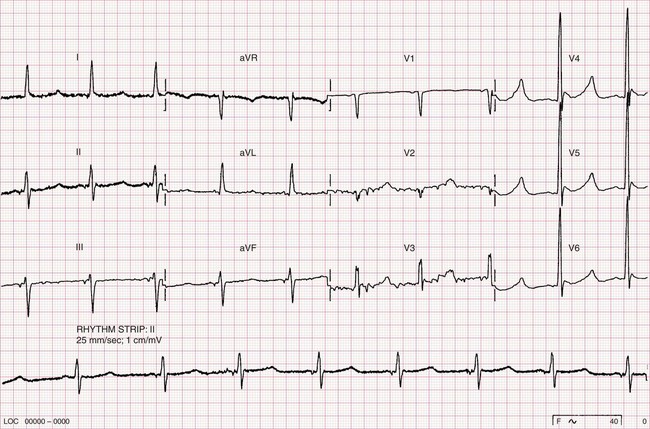
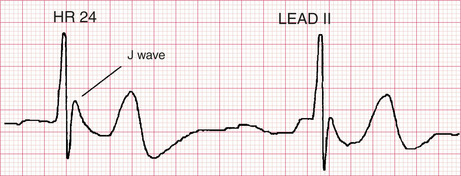
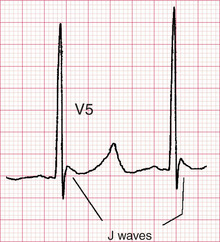
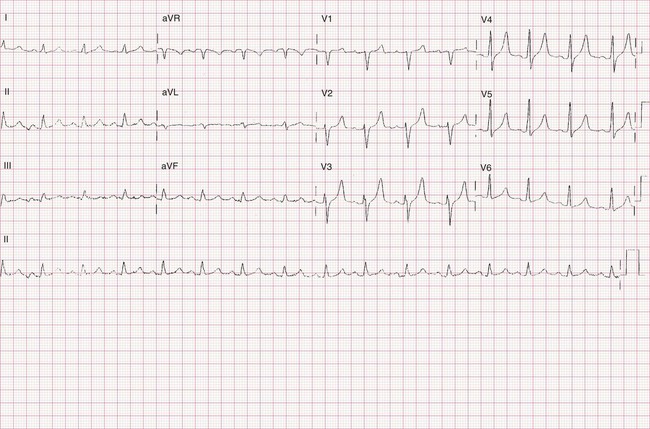
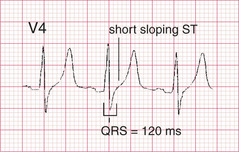
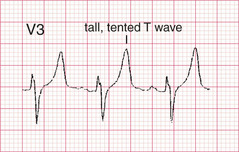
Section 8 Systemic disorders and drug effects Hypothermia Hyperkalaemia (subtle ECG changes) Hyperkalaemia (extreme ECG features) Hypokalaemia Hypocalcaemia Hypercalcaemia Digoxin (digitalis) effect Tricyclic antidepressant overdose Case 76 A thin 79-year-old lady found on the floor at home Hypothermia • Bradycardia. • Prominent deflection at the junction of QRS and ST segment (J wave): – an extreme example, from another patient, is shown in Fig. 76.1, temperature = 26°C. • Increased ventricular activation time. • Long QT interval. • Shivering artifact. Fig. 76.1 Hypothermia. Extreme J waves from another case. Features of this ECG • Bradycardia, 48 b.p.m. • Prominent J waves in leads V4-6 (Fig. 76.2) • A shivering artifact is seen in leads V2 and V3. • Left anterior hemiblock: – left axis deviation −36° – initial R waves in the inferior leads Fig. 76.2 J waves. Clinical Note This lady had a core temperature of 27°C. Case 77 A 58-year-old man with chronic liver disease Hyperkalaemia (subtle ECG changes) • Small or absent P waves. • Long PR interval. • Broad QRS complexes especially the terminal component. • Decreased R wave size. • Axis deviation. • Shortened or absent ST segment. • Tall tented T waves (usually the earliest ECG manifestation of hyperkalaemia). • Atrial fibrillation. • Ventricular fibrillation. Features of this ECG • Sinus rhythm, 98 b.p.m., normal QRS axis (+50°) • Small P waves • QRS duration of 120 ms, upper limit of normal (Fig. 77.1) • Short, upsloping ST segment (Fig. 77.1) • Tall tented T waves (Fig. 77.2) Fig. 77.1 Lead V4. Fig. 77.2 Lead V3. Common causes of hyperkalaemia → Increased potassium release from cells: – metabolic acidosis – insulin deficiency – trauma – tumour lysis – digoxin overdose → Reduced urinary excretion: – acute or chronic renal failure – drugs (potassium sparing diuretics, ACE inhibitors, ciclosporin, tacrolimus) – hypoaldosteronism Clinical Note This man had alcoholic cirrhosis. He was on spironolactone (a potassium sparing diuretic) to treat ascites and oedema. He had over diuresed and was admitted with dehydration and renal failure. Serum potassium was 7.5 mmol/L. Case 78 A 52-year-old man with marked weakness of both arms and legs Hyperkalaemia (extreme ECG features) • Small or absent P waves. • Long PR interval. • Atrial fibrillation. • Broad QRS complexes especially the terminal component. • Decreased R wave size. • Axis deviation. • Shortened or absent ST segment. • Tall tented T waves (‘they would hurt if you sat on them!’). • Ventricular fibrillation. Features of this ECG • Indeterminate rhythm, 90 b.p.m., right axis deviation • Broad, bizarre complexes (Fig. 78.1) Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Hypertrophy patterns Bundle branch block Ventricular rhythms Ischaemic heart disease Stay updated, free articles. Join our Telegram channel Join Tags: ECGs by Example Aug 29, 2016 | Posted by admin in CARDIOLOGY | Comments Off on Systemic disorders and drug effects Full access? Get Clinical Tree
Section 8 Systemic disorders and drug effects Hypothermia Hyperkalaemia (subtle ECG changes) Hyperkalaemia (extreme ECG features) Hypokalaemia Hypocalcaemia Hypercalcaemia Digoxin (digitalis) effect Tricyclic antidepressant overdose Case 76 A thin 79-year-old lady found on the floor at home Hypothermia • Bradycardia. • Prominent deflection at the junction of QRS and ST segment (J wave): – an extreme example, from another patient, is shown in Fig. 76.1, temperature = 26°C. • Increased ventricular activation time. • Long QT interval. • Shivering artifact. Fig. 76.1 Hypothermia. Extreme J waves from another case. Features of this ECG • Bradycardia, 48 b.p.m. • Prominent J waves in leads V4-6 (Fig. 76.2) • A shivering artifact is seen in leads V2 and V3. • Left anterior hemiblock: – left axis deviation −36° – initial R waves in the inferior leads Fig. 76.2 J waves. Clinical Note This lady had a core temperature of 27°C. Case 77 A 58-year-old man with chronic liver disease Hyperkalaemia (subtle ECG changes) • Small or absent P waves. • Long PR interval. • Broad QRS complexes especially the terminal component. • Decreased R wave size. • Axis deviation. • Shortened or absent ST segment. • Tall tented T waves (usually the earliest ECG manifestation of hyperkalaemia). • Atrial fibrillation. • Ventricular fibrillation. Features of this ECG • Sinus rhythm, 98 b.p.m., normal QRS axis (+50°) • Small P waves • QRS duration of 120 ms, upper limit of normal (Fig. 77.1) • Short, upsloping ST segment (Fig. 77.1) • Tall tented T waves (Fig. 77.2) Fig. 77.1 Lead V4. Fig. 77.2 Lead V3. Common causes of hyperkalaemia → Increased potassium release from cells: – metabolic acidosis – insulin deficiency – trauma – tumour lysis – digoxin overdose → Reduced urinary excretion: – acute or chronic renal failure – drugs (potassium sparing diuretics, ACE inhibitors, ciclosporin, tacrolimus) – hypoaldosteronism Clinical Note This man had alcoholic cirrhosis. He was on spironolactone (a potassium sparing diuretic) to treat ascites and oedema. He had over diuresed and was admitted with dehydration and renal failure. Serum potassium was 7.5 mmol/L. Case 78 A 52-year-old man with marked weakness of both arms and legs Hyperkalaemia (extreme ECG features) • Small or absent P waves. • Long PR interval. • Atrial fibrillation. • Broad QRS complexes especially the terminal component. • Decreased R wave size. • Axis deviation. • Shortened or absent ST segment. • Tall tented T waves (‘they would hurt if you sat on them!’). • Ventricular fibrillation. Features of this ECG • Indeterminate rhythm, 90 b.p.m., right axis deviation • Broad, bizarre complexes (Fig. 78.1) Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Hypertrophy patterns Bundle branch block Ventricular rhythms Ischaemic heart disease Stay updated, free articles. Join our Telegram channel Join Tags: ECGs by Example Aug 29, 2016 | Posted by admin in CARDIOLOGY | Comments Off on Systemic disorders and drug effects Full access? Get Clinical Tree