3 Suggested Views for Fetal Heart Imaging
I. ASSESSMENT OF FETAL LIE
C. Left–right orientation
1. Once the fetal lie is determined by demonstrating the long-axis of the fetus, one can identify the left and right sides of the fetus.
2. For consistency, the long axis can be demonstrated with the notch on the transducer positioned toward the head of the fetus.
3. Rotating 90 degrees clockwise to obtain the short-axis image through the fetus when supine, one can display the left of the fetus to the right of the screen and the right to the left of the screen. The reverse is true when the fetus is prone.
II. CROSS-SECTIONAL IMAGES
Once fetal lie is established, a short-axis or axial image through the fetal chest can be obtained.
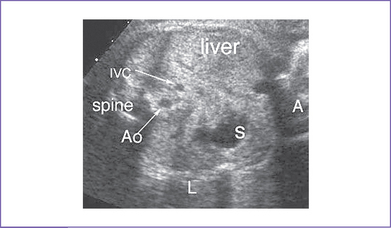
A. Assessment of visceral and atrial situs
Sweeping to the abdomen: The more rightward liver, leftward stomach, and posterior spleen, as well as the position of the descending aorta and inferior vena cava (IVC) can be demonstrated (Fig. 3-1).
B. Umbilical vein and artery (SEE CHAPTER 1)
1. Sweeping toward the feet of the fetus: The insertion of the umbilical vessels into the fetal abdomen can be demonstrated.
2. The two umbilical arteries course farther caudally around the fetal bladder to join the left and right iliac arteries.
3. The umbilical vein can be followed as it courses through the fetal liver in a cephalad direction.
C. Systemic veins
1. Ductus venosus: Where the umbilical vein has a sudden change in its diameter and by color there is a sudden increase in flow velocities, the ductus venosus joins the hepatic venous and IVC flow, which heads toward the heart.
2. Hepatic veins: At least one left and one right hepatic vein can usually be demonstrated connecting with the IVC, often very close to the insertion of the IVC into the inferior portion of the right atrium.
3. IVC: Lower in the fetal body, the IVC begins in a more posterior position. As it courses cephalad, however, it courses anteriorly to meet the right atrium.
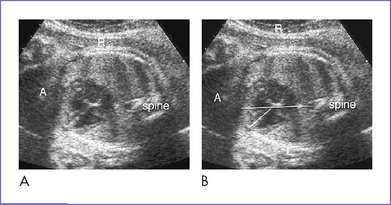
D. The four-chamber view
The four-chamber view (Fig. 3-2) is obtained with a cross-sectional image through the fetal chest.
1. The position of the heart is usually largely in the left chest, with only a portion of the right atrium positioned just to the right of the midline.
2. The size of the heart is usually about one third the size of the thorax.
3. The axis of the heart is determined by drawing a line from the spine to the sternum (as 0 degrees) and using the septal position to determine the angle. Normally the axis is 40 degrees. Any deviation of this axis could suggest cardiac or extracardiac (particularly intrathoracic) pathology.
a. The left atrium is the most posterior chamber.
b. It lies posterior and largely to the left of the midline just in front of the descending aorta.
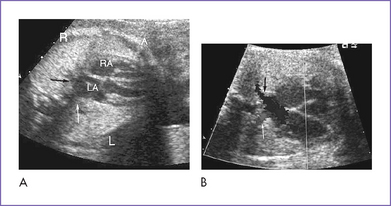
5. Pulmonary veins (Fig. 3-3).
a. The left and right pulmonary veins course around the descending aorta from each lung to join the posterior wall of the left atrium; at least one of each should be shown.
b. The upper pulmonary veins course immediately inferior to the respective branch pulmonary arteries (PAs).
a. The right atrium lies to the right of the midline and anterior relative to the left atrium.
b. The atria should be symmetric.
a. The atrial septum consists of the septum secundum, the septum primum, and the atrioventricular (AV) septum, which is the most anterior aspect of the septum near the AV valves. The atrial septum is best seen by imaging perpendicular to its plane.
b. The foramen ovale is a communication in the atrial septum that is partially covered by the septum primum. Its flow orifice is roughly the same size as the aortic valve.
c. The coronary sinus is a small tubular structure that courses along the inferior portion of the left atrium, just above the posterior AV ring. It may be dilated if there is a persistent left superior vena cava (SVC) that connects and returns to it.
a. The AV valves are usually offset, with the septal leaflet hinging closer toward the ventricular apex. Earlier in gestation the offset is not as dramatic.
b. The thin, bileaflet mitral valve has no septal attachments (“septophobic”), but rather opens toward the free wall of the left ventricle (LV).
c. In a four-chamber view, one cannot clearly demonstrate the three thin leaflets of the tricuspid valve without sweeping. The valve opens toward the apex of the right ventricle (RV) and has septal attachments as a result of the septal leaflet (“septophilic”).
10. Interventricular septum: With sweeps through the ventricular septum, all components of the septum can be evaluated.