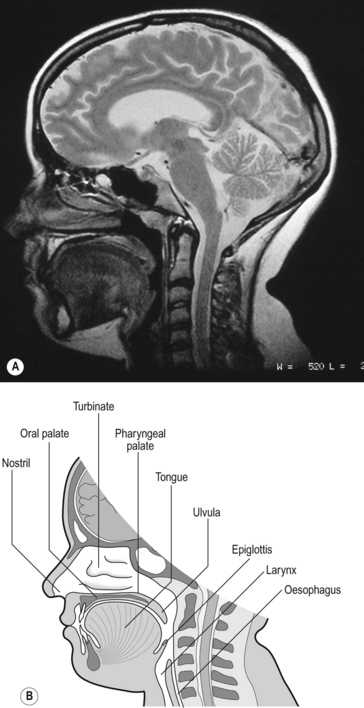
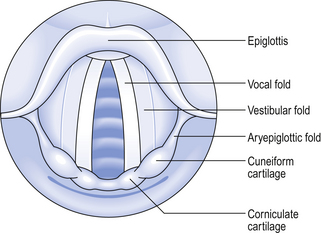
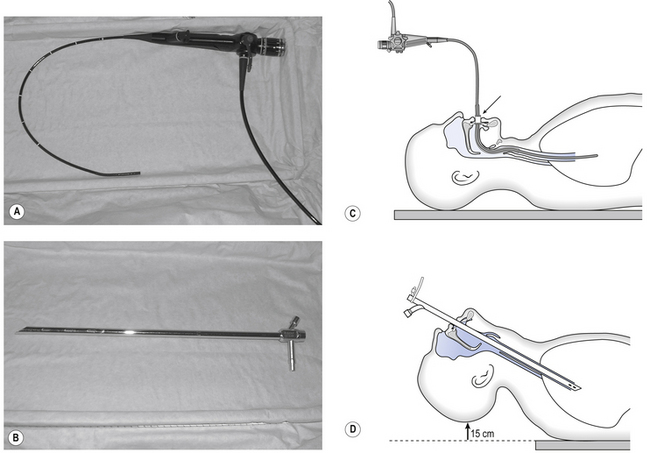
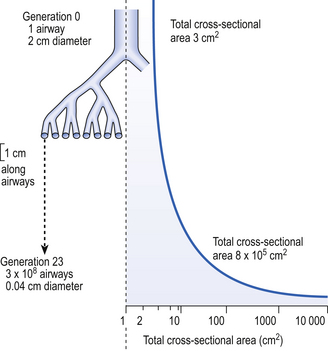
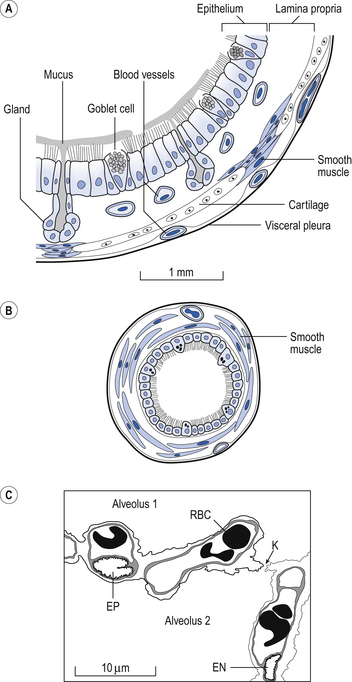
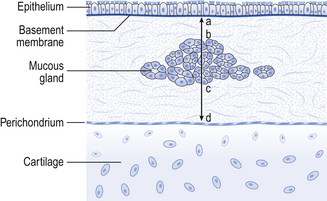
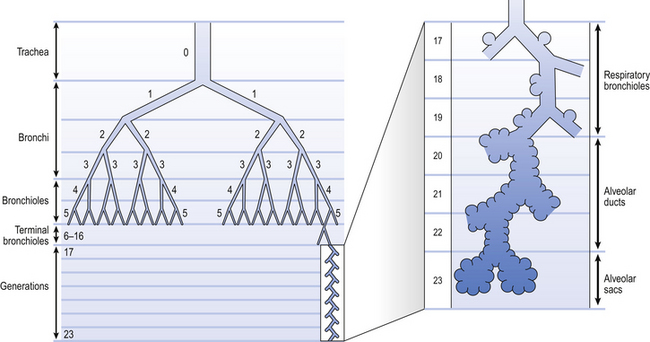
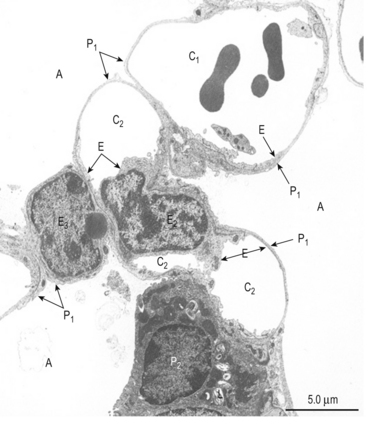
2 We will first describe the airways of the lung and then the tissues that surround them. The structures of the upper airways are clearly seen in a paramedial sagittal section of the head and neck (Fig. 2.1). Much more sinister and life-threatening than rhinitis is obstructive sleep apnoea (OSA; apnoea = absence of breathing). This should not be confused with central sleep apnoea, where the patient ceases to make respiratory efforts while they are sleeping. In OSA the patient’s attempts to breathe are physically obstructed by anatomical and physiological peculiarities of the upper airways. In Figure 2.1 the subject is breathing through his nose because the lips are closed and the tongue lies against the palate. When you breathe through the mouth – for example when you blow out a candle or suck through a straw – the soft palate is arched upward to form a seal against Passavant’s ridge at the top of the pharynx. This form of airways obstruction is a normal function. Similarly, under normal circumstances, the genioglossus muscle of the tongue has a high resting tone in conscious subjects, and this holds the tongue forward, preventing it from obstructing the airway. During sleep, and particularly in those suffering from the dangerous condition of obstructive sleep apnoea, the tongue falls against the back wall of the pharynx and obstructs breathing. The muscle tone of the pharynx itself becomes reduced, particularly during REM (rapid eye movement) sleep and in OSA the pharynx collapses under the negative pressure of inspiration. Blocking of the airways by the tongue also and almost inevitably occurs during general anaesthesia and requires immediate attention from the anaesthetist. In humans the nose extends from the nostrils (external nares) to the choanae (internal nares), which empty into the nasal part of the pharynx. Each nostril narrows to form its nasal valve, and at this level the total cross-sectional area of the airways is narrower (3 mm2) than anywhere else in the system. This narrowing imposes the majority of the high resistance to airflow found in the nose (see Chapter 5) and, combined with the sharp turn the inspiratory air must make as it enters the wide (140 mm2) lumen of the cavum of the nose, causes turbulence. The walls of the nasal cavum are rigid bone projecting out into the airway from the lateral walls as the turbinates. These have a large surface area (150 cm2) covered by vascular mucosal erectile tissue important in the ‘air-conditioning’ activities of the nose. This mucosal tissue can swell considerably in conditions such as rhinitis (described above), and it is here that nasal decongestants such as oxymetazoline, an agonist of α adrenergic receptors on vascular smooth muscle, act to clear a blocked nose by causing the vascular smooth muscle to contract. The major function of the upper airway is to air-condition the inspirate. It is not essential to breathe through the nose to do this, and the mouth will make a fairly good job of warming and humidifying inhaled air before it reaches the larynx. However, the mouth has not evolved for that purpose and the unpleasant consequences of using it are well known to anyone who has had to breathe through their mouth because a cold has obstructed their nasal airways. The larynx (see Fig. 2.1) is in fact a rather complicated box made up of plates of cartilage. It can be closed off by drawing together the two curtains of muscle which make up the vocal folds across the lumen of the larynx. Effective coughs depend on the closure and rapid opening of these ‘curtains’, which under less extreme circumstances are used to produce and modify the sounds that make up speech. The vocal folds can be drawn together so strongly that they are airtight against the greatest efforts to breathe the subject can make. This is clearly a ‘bad thing’ and can occur accidentally when an anaesthetist is trying to get an endotracheal tube into a patient’s trachea. This dangerous closing of the larynx is called laryngospasm. A picture of what an anaesthetist would see when approaching the larynx is shown in Fig. 2.2. It is frequently useful to inspect the airways below the larynx. First the trachea (part of which is extrathoracic), and then the intrathoracic airways. The instrument used for this is called a bronchoscope and may be of the rigid ‘open tube’ type through which the airways are inspected, or the flexible fibreoptic variety (Fig. 2.3) which, as well as providing a view of the inside of the airways through its fibreoptic system, contains channels through which a variety of sampling and surgical instruments may be passed. Each type of bronchoscope has its advantages, but 95% of bronchoscopic procedures carried out these days are fibreoptic. Biopsy forceps, brushes and needles, balloon catheters and laser fibres can all now be passed through flexible bronchoscopes to carry out procedures after an initial inspection of even very small intrathoracic airways. The airways of the lungs are often referred as the bronchial tree, and casts in which the airways are filled with plastic material and then the tissues dissolved away look like a deciduous tree in winter. The branches of this ‘tree’ can be represented in diagrammatic form as the ‘generations’ of a family tree (Fig. 2.4). In some bronchitic patients secretions sometimes fill small airways, solidify, and are coughed up as small ‘casts’ of part of this ‘tree’. Fig. 2.4 The naming of airways. There is of course a gradual change in structure from one type of airway to another. One particular type of airway can occur at different distances into the lungs. (After Weibel, 1963) The trachea is the first and largest of about 23 generations of airways. The airways of each generation arise from the previous one by a system of irregular dichotomous branching airways. Dichotomous because each ‘mother’ airway gives rise to two ‘daughter’ airways, and irregular because the daughters, although smaller than the mother, are not necessarily of equal size. The naming of these generations is illustrated in Figure 2.4, from which it may not be obvious that the number of airways (N) in a generation (Z), (counting the single trachea as generation 0) is: The effect of dichotomous branching of individual airways on the total cross-sectional area (the sum of the cross-sectional areas of all the airways at that level) is remarkable and is shown in Figure 2.5. Notice that ‘Total cross-sectional area’ is measured on a log scale, and so this value increases much more than it appears to in the figure. The functional consequences of this increase are profound because it causes the velocity of the air to fall rapidly as it moves into the lung. This effect is discussed in more detail in Chapter 5. The dimensions of some of the airways that make up the bronchial tree are given in Table 2.1. As you go deeper into the lung the transitional and respiratory generations of the airways bear more and more alveoli until the alveolar sacs are totally made up of them. Alveoli do not look like the bunches of grapes or balloons stylistically represented in many textbooks, but rather pock-marked cavities with holes (pores of Kohn, K in Fig. 2.7C) between many adjacent alveoli and with macrophages wandering over their surface ready to engulf and digest foreign particles (see Figs 2.6, 2.17). Fig. 2.6 Scanning electron micrograph of an alveolus. A, alveolus; C1, C2, C3, capillaries; E, endothelial cell; P1, type I pneumocytes; P2 type II pneumocyte; L, lamellar bodies. From Young and Heath 2000. The microscopic structure of the wall of the airways changes as you go deeper into the lungs. Three ‘snapshots’ of airway wall structure are shown in Figure 2.7 but of course the structure changes gradually from generation to generation. • The inner mucosal surface consists of ciliated epithelium and underlying mucus-secreting goblet cells. The activity of the cilia and the secretions of the globlet cells make up the mucociliary escalator (see Air-conditioning, below), which is important in removing inhaled particles in the lungs. • Outside the mucosal layer comes a smooth muscle layer in which the fibres are in continuous bundles. This smooth muscle is found in decreasing amounts from the largest airways right down to the entrances to the alveoli. • The outermost layer is of connective tissue, which in the large bronchi contains supporting cartilage. As the airways penetrate the lung they first lose their cartilage support and smooth muscle occupies a greater percentage of the airway wall. Then the ciliated epithelium becomes the squamous type, finally forming the respiratory region of the lung. The arrangement representing bronchial structure illustrated in Figure 2.7 and described above is modified in chronic bronchitis in a way that provides a histopathological quantitative diagnosis of the disease. The Reid Index provides a measure of proportion of bronchial glands to total wall thickness (Fig. 2.8). In normal lungs mucous glands occupy less than 40% of total wall thickness. In chronic bronchitis this proportion is altered by hyperplasia of the glands. A characteristic of chronic bronchitis is an increase in the products of these glands. One of the characteristics of the respiratory surface of any animal is that it should be thin, offering minimal separation between the outside medium (air or water) and the blood. This is beautifully demonstrated in the lungs, which are the only place in our body where blood capillaries come into direct contact with the outside air, as a result of the fusion of the type I epithelial cells (which make up about 95% of the lining of the respiratory zone; Fig. 2.6) with the pulmonary capillary endothelium. This fusion results in an ultrathin layer ideal for the diffusion of gas but not much good for support. Evolution has resulted in this thinning occurring on only one side of the pulmonary capillaries, whereas the cells on the other side remain separate and more robust, supporting the capillary in its place (Fig. 2.9).
STRUCTURE OF THE RESPIRATORY SYSTEM, RELATED TO FUNCTION
Introduction
The upper airways
Mouth and nose – rhinitis, the common cold and obstructive sleep apnoea
The larynx – intubation of the airways
Bronchoscopy
The intrathoracic airways

Histological structure of the airways
Bronchitis and the Reid Index
The respiratory region
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


STRUCTURE OF THE RESPIRATORY SYSTEM, RELATED TO FUNCTION