CHAPTER 11
Stage D Heart Failure: Options and Opportunities
“Diseases desperate grown / By desperate appliance are relieved / Or not at all.”
–William Shakespeare, Hamlet, Act IV, Scene 3
Who Is the Stage D Heart Failure Patient?
Stage D heart failure, also known as advanced heart failure, represents the group of patients with refractory symptoms that fail to stabilize despite hospital admission. Identifying when a patient has crossed the threshold to advanced heart failure can be challenging. Families or caregivers may have difficulty recognizing gradual changes in physical and mental status. Nevertheless, the occurrences of multiple hospital admissions, cardiorenal syndrome, the need to reduce doses of neurohormonal blocker medications, recurrent ventricular arrhythmias, and laboratory markers of disease progression, including hyponatremia or anemia, may herald a shift to advanced disease and poor prognosis.1 The need for chronic inotropic support implies a particularly poor prognosis (Figure 11.1). Patient frailty and the lack of psychosocial support further reduce the ability of these patients to cope with both cardiac and noncardiac limitations. Aggressive measures such as heart transplant or left ventricular assist device are more likely to benefit the Stage D patient whose overall disability is predominantly due to heart failure alone. When there is multisystem involvement, palliative care may be more appropriate.
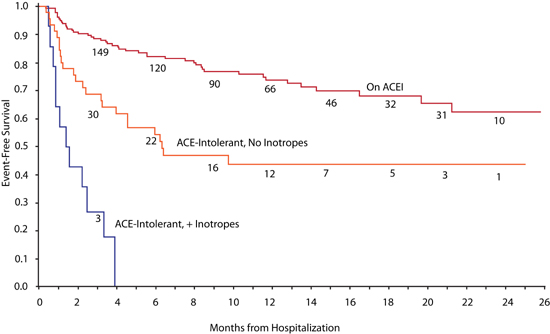
FIGURE 11.1 Heart failure mortality for patients dependent on chronic inotropic support. ACE inhibitor intolerance and a need for inotropes both identify heart failure patients with a worse prognosis.2 Source: Adapted with permission from Kittleson et al., J Am Coll Cardiol. 2003;41(11):2029-2035.
Stage D patients, in general, have symptoms at rest or with simple activities of daily living and a poor 1-year prognosis. Several clinical criteria suggest that heart failure has progressed to Stage D (List 11.1). Most patients have been hospitalized for heart failure in the preceding 12 months. Even for the Stage D patient, a careful evaluation is warranted to confirm the diagnosis of heart failure as the etiology of a patient’s symptoms. Precipitating factors should be identified and, if possible, treated. The measures that have been outlined for patients in Stages A, B, and C should be reviewed for potential treatment options.
LIST 11.1 Clinical Criteria that Suggest Stage D
Palliative Care
Palliative care should be considered for patients with severe, persistent symptoms who do not qualify for or do not desire ventricular replacement options, such as heart transplantation or left ventricular assist devices. Palliative care is associated with improved patient and family satisfaction in care and symptom management and decreased hospital readmissions, procedures, interventions, and cost.4 Palliative care includes many treatments not usually considered as part of heart failure care (Table 11.1). Consultations for palliation may result in referral to hospice that will usually be an at-home program. Surprisingly, in advanced heart failure patients, hospice has been associated with an increase in survival compared to those who did not receive hospice care.4
TABLE 11.1 Palliative Therapies for Stage D Symptoms.4
CLASS OF RECOMMENDATIONS* | |||||
SYMPTOMS | I | IIA | IIB | III | INSUFFICIENT |
DYSPNEA | Loop diuretics with or without thiazides Nitrates Low-dose opioids | Inotropes Ultrafiltration (if diuretic resistant) Walking aids Breathing training Exercise training Hawthorn extract | Oxygen (without hypoxia) | Benzodiazapines | Acupuncture/ acupressure |
PAIN | Opioids Bone pain: bisphosphonates Anginal pain: nitrates, β blockers, Ca2+ channel blockers, ranolazine, coronary revascularization | Acupuncture Exercise training Music | Nonsteroidal anti-inflammatory drugs | ||
DEPRESSION | Selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, tricyclic antidepressants | Psychological interventions: cognitive behavioral therapy, counseling, or supportive therapy | Exercise | Acupuncture | |
FATIGUE | Treat secondary causes (anemia, infection, sleep apnea, etc) Stimulants Exercise training Hawthorn extract | Increased rest and reduction of physical activity | Anti-inflammatory agents L-carnitine Nutritional supplements or appetite stimulants | ||
*Recommendations for palliative care based on Benefit compared to Risk of Treatment:
Class I: Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective.
Class IIa: The weight of evidence or opinion is in favor of the procedure or treatment.
Class IIb: Usefulness/efficacy is less well established by evidence or opinion.
Class III: Conditions for which there is evidence and/or general agreement that the procedure or treatment is not useful/effective and in some cases may be harmful.
Insufficient: Insufficient evidence to make recommendation.
Cardiac Transplant
Cardiac transplant has become a widely accepted treatment for advanced heart disease. Even so, the psychosocial requirements and long term immunosuppressive therapy associated with the procedure require careful patient selection and preparation.
REFERRAL OR CONSIDERATION FOR CARDIAC TRANSPLANT
Consider patients for evaluation for cardiac transplant when they develop Stage D findings—despite comprehensive Stage C therapies. Significant noncardiac comorbidities or inability to comply with a complex medical regimen may contraindicate transplant. Most cardiac transplant candidates are 70 years or younger in age.
One clinical finding in particular suggests the need for transplant evaluation. The occurrence of cardiac cachexia defined as a nonintentional weight loss of at least 7.5% over six months is an ominous finding associated with a 39% one-year mortality5 and an independent risk factor for death.
Measurement of patient oxygen consumption during cardiopulmonary exercise testing (see Chapter 2) can provide useful prognostic information to aid with the timing of listing for cardiac transplant. A peak O2 consumption of ≤ 14 mL/kg/min can indicate a poor one-year prognosis with only continued medical therapy and no cardiac transplant (Figure 11.2).6 Especially in patients younger than 40 years old, percent predicted peak O2 consumption (PPVO2) may be more accurate.7 In these patients, the finding of a PPVO2 (corrected for age, body weight, and sex) ≤ 50% is a worse prognostic indicator than using a fixed value threshold of ≤ 14 mL/kg/min (Figure 11.3). Conversely, a PPVO2 > 50% has been associated with a one- and two-year survival of 98% and 90%, respectively. Both peak O2 consumption and PPVO2 can be used in clinical practice.
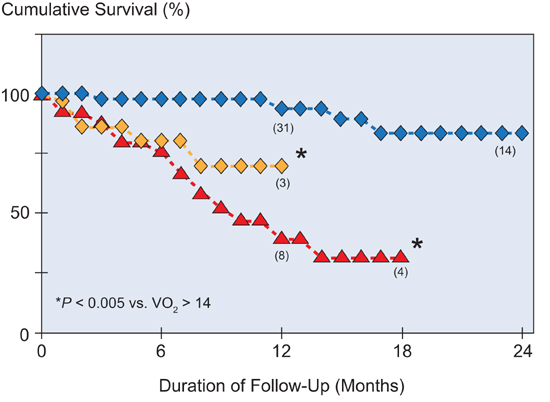
FIGURE 11.2 Cardiopulmonary exercise testing: Peak VO2 and prognosis. A peak VO2 value of ≤ 14 mL/kg/min (red triangles and yellow diamonds) predicts a poor survival. Some patients were accepted as transplant candidates (yellow diamonds [n = 35]) and some patients were rejected for transplant (red triangles [n = 27]). Patients with VO2 > 14 mL/kg/min (blue diamonds [n = 52]) were not considered for transplant.6 Source: Adapted with permission from Mancini et al., Circulation. 1991;83(3):778-786.
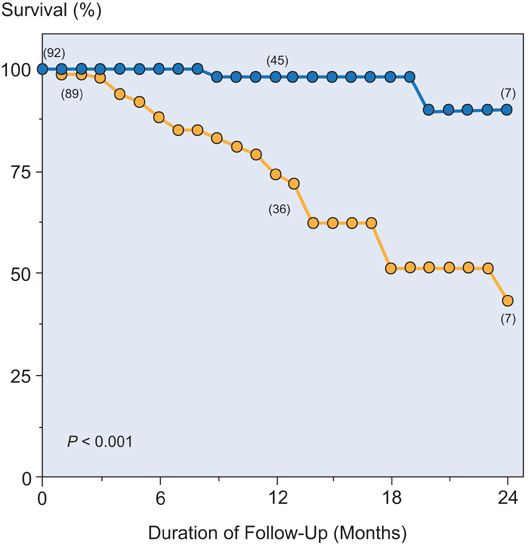
FIGURE 11.3 Percent predicted peak O2 consumption (PPVO2) as a determinant of prognosis in younger patients. Those with a PPVO2 ≤ 50% (yellow [n = 89]) had a poor prognosis compared to those with a PPVO2 > 50% (blue [n = 92]).7 Source: Adapted with permission from Stelken et al., J Am Coll Cardiol. 1996;27(2):345-352.
Because heart failure patients have reduced exercise capacity, the modified Naughton treadmill protocol (which increases workload at a slower rate than the standard Bruce protocol) may give a better estimate of peak oxygen consumption. In the modified Naughton protocol, each stage increases estimated O2 consumption by 1 MET (3.5 mL O2/kg/min) (Table 11.2).
TABLE 11.2 Example of modified Naughton protocol useful for exercise testing in patients with heart failure. Stage X of this protocol is equivalent to Stage 3 of the Bruce Protocol.10
STAGE (2-MINUTE INCREMENTS) | SPEED (MPH) | GRADE (%) |
I | 1.0 | 0 |
II | 1.5 | 0 |
III | 2.0 | 3.5 |
IV | 2.0 | 7.0 |
V | 2.0 | 10.5 |
VI | 3.0 | 7.5 |
VII | 3.0 | 10.0 |
VIII | 3.0 | 12.5 |
IX | 3.4 | 12.0 |
X | 3.4 | 14.0 |
Treadmill testing can also provide a baseline index for the amount of functional improvement a patient can expect after heart transplant based on the assessment of oxygen consumption and duration of graded exercise in patients with heart failure.8,9
FUNCTIONAL RECOVERY AFTER HEART TRANSPLANT
Improvement in functional capacity is an important aspect of quality of life after heart transplant. The majority of patients are NYHA class IV at the time of heart transplant.
After transplant, most patients are returned to a New York Heart Association class I functional status, although peak exercise capacity and oxygen consumption are still less than matched controls.9 On average, peak O2 consumption with exercise improves over the first 6 months after heart transplantation.9 Greater increases in peak O2 consumption will be achieved by patients who participate in a structured cardiac-rehabilitation program.11
Following heart transplant, patients have an increased resting heart rate of 80–120 bpm. This reflects the denervated state of the heart and the absence of parasympathetic innervation that normally lowers the resting heart rate. Nevertheless, with exercise, further increases in heart rate are achieved by the delivery of catecholamines to the heart via the circulation. In a multivariate analysis, younger age, higher peak heart rate, lower body mass index, and better diastolic function were independent predictors of peak O2 consumption with exercise after transplant.12 In younger recipients without significant comorbidities, remarkable physical endurance achievements can be achieved (Figure 11.4).

FIGURE 11.4 Functional recovery after heart transplant. Three heart transplant recipients (ages 52, 29, and 45 years) after completing the first of 3 half marathons in 2012. Recipients were 1.8, 2.8, and 3.3 years post heart transplant, respectively.
< div class='tao-gold-member'>



