
Fig. 9.1
Liver cirrhosis, consequence of a nodular regenerative hyperplasia, complicated by hypersplenism with thrombopenia (platelets 28,000 G/l), and bleeding esophageal varices. A restoration of the platelet count is researched. (a) CT frontal reconstruction: splenomegaly. (b) Splenomegaly, large splenic vein. (c) Large diameters of portal vein and its branches. (d) Celiac trunk (CT) selective angiogram: large and sinuous splenic artery. (e) Distal splenic A hyperselective catheterization (microcatheter): modal pattern in bifurcation; microaneurysms. (f) Hyperselective catheterization of the lower terminal branch, which has been occluded with microparticles, and then catheterization and occlusion of the lower branch of the superior terminal branch. At the end of this procedure, 4 cm3 of 300–500 μm diameter particles, and then 3 cm3 of 500–700 μm diameter, and finally 1 cm3 of 900–1,200 μm diameter have been injected, in order to observe a considerable slowing of the flow in these branches. (g) The upper pole of the spleen has not been embolized. (h) CT, 1 month later: 60–70 % devascularization of the splenic parenchyma. During the immediate follow-up: moderate fever (38 °C), limited pleural effusion, and platelet count progressively arising (from 28 × 103 to 109 × 103 G/l) without any pancreatic enzymes movement
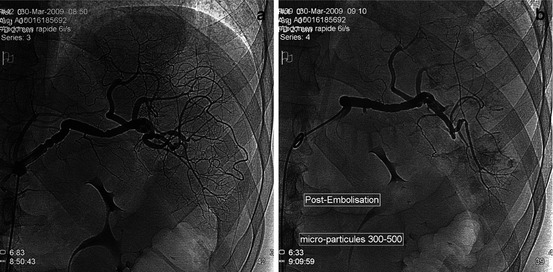
Fig. 9.2
45-year-old M, HCC on VHC cirrhosis, waiting for hepatic transplantation, with a iatrogenic thrombopenia (antiviral treatment). The association of a splenic embolization to a TACE has been proposed. (a) Splenic A selective angiogram: moniliform and large splenic A, splenomegaly. (b) Control angiogram after a partial embolization of the lobar inferior branch of the splenic A (microparticles, 300–500 μm 3 cm3 and then 700–900 μm 1 cm3)
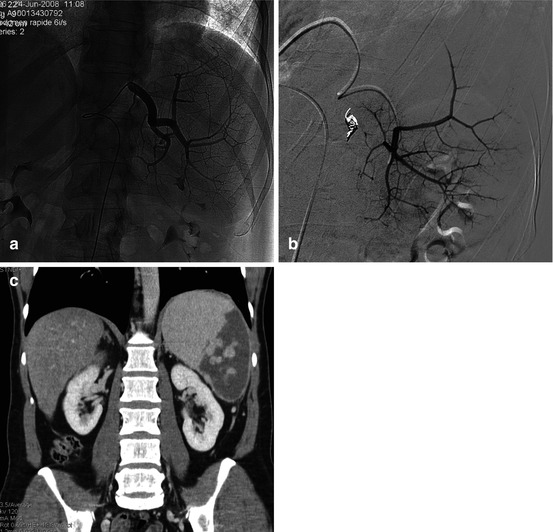
Fig. 9.3
Alcoholic and post-HVC cirrhosis, with hypersplenism and thrombopenia (platelets 16,000 G/l). (a) Selective catheterization of the splenic A. (b) After exclusion (microparticles + coils) of the inferior lobar branch of the splenic A, the remaining functional splenic parenchymal volume looks important. A complementary embolization of a part of the superior lobar A parenchyma was decided: hyperselective angiogram of this territory before embolization. (c) No clinical adverse event during the first month follow-up; platelets 81,000 G/l
Appendix: AAST Classification (Spleen) [1]
Gradea | Injury type | Injury description | AIS |
|---|---|---|---|
I | Hematoma | Subcapsular <10 % surface area | 2 |
Laceration | Capsular tear <1 cm parenchymal depth | 2 | |
II | Hematoma | Subcapsular, 10–50 % surface area; intraparenchymal, <5 cm in diameter
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|