Chapter 3 Specialized Electrodiagnostic Studies
LATE RESPONSES
Late responses are obtained using special techniques that are not possible with conventional nerve conduction studies. The settings are usually changed to allow the examiner to capture these responses. This include using longer sweep speed of 5–10 ms/division and lower amplifier gain of 200–500 μV/division which could be adjusted depending on the limb studied, site of stimulation and magnitude of response. Since it is intended for the action potentials to travel proximally with the late response recording, the bipolar stimulator is switched to place the cathode more proximally and the anode distally.
F Wave
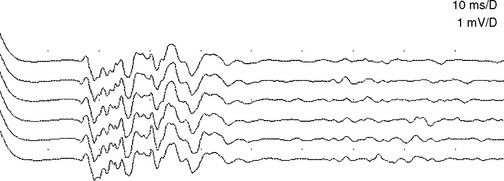
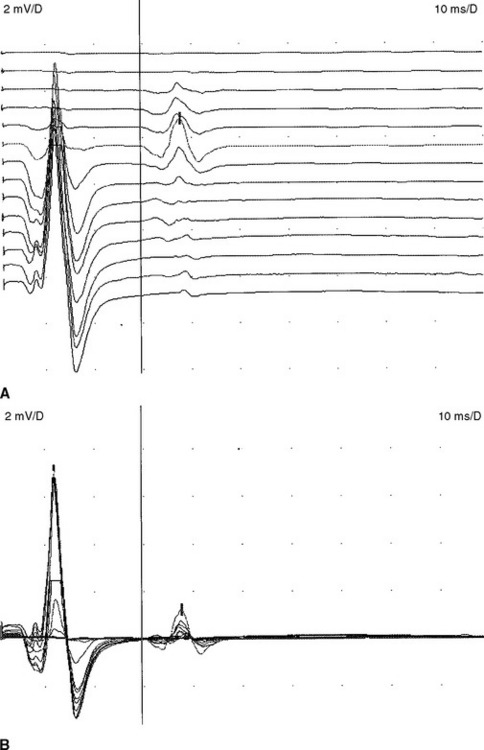
The F waves are low-amplitude and ubiquitous responses that are typically variable in latency, amplitude, and morphology (Figure 3-1A and B). Their variability is explained by differing groups of motor neurons generating the recurring discharge with each individual group of neurons having different number of motor neurons and conducting properties. Several parameters may be analyzed, but the minimal F wave latency is the most reliable and useful measurement since it represents conduction of the largest and fastest motor fibers. Since F wave latencies vary from one stimulus to the next, an adequate study requires that about 10 F waves be clearly identified. The minimal F wave latency is also dependent on the length of motor axons which correlates with the patient’s height and limb length. The most sensitive criterion of abnormality in a unilateral disorder is a latency difference between the two sides, or between two similar nerves in the same limb. Absolute latencies are most useful only for sequential reassessment of the same nerve. F wave persistence is a measure of the number of F waves obtained for the number of stimulations. This varies between individuals and is inhibited by muscle activity while it is enhanced by relaxation or the use of Jendrasik maneuver. It is usually above 50% except when stimulating the peroneal nerve while recording the extensor digitorum brevis. F wave chronodispersion is the degree of scatter among consecutive F waves and is determined by the difference between the minimal and maximal F wave latencies. It indicates the range of motor conduction velocities between the smallest and largest myelinated motor axon in the nerve. The F wave conduction velocity may be calculated after distal and proximal supramaximal stimulations and provides a better comparison between proximal and distal (forearm or leg) segments.
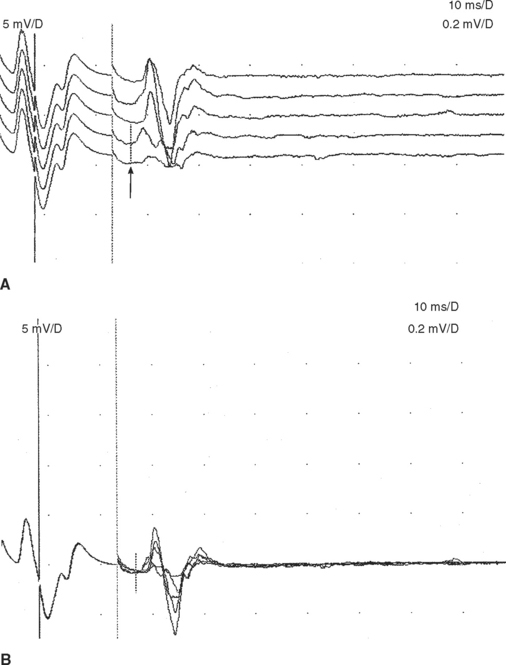
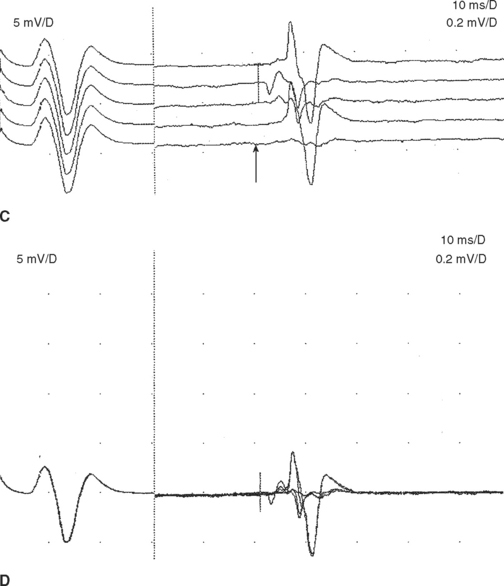
F wave latencies are prolonged in most polyneuropathies, particularly the demyelinating type, including Guillain-Barré syndrome and chronic inflammatory demyelinating polyneuropathy (CIDP) (Figure 3-1C and D). F wave latencies in radiculopathies have a limited use. They may be normal despite partial motor axonal loss because the surviving axons conduct normally, and in single radiculopathies since most muscles have multiple root innervation. Finally, focal slowing at the root level may get diluted by the relatively long motor axon.
A Wave
The A wave (axonal wave) is a potential that is seen occasionally during recording of F waves at supramaximal stimulation. The A wave follows the CMAP and often precedes, but occasionally follows, the F wave. The A wave may be mistakenly considered for an F response but its constant latency and morphology in at least 10 out of 20 stimulations differentiates it from the highly variable morphology and latency of the F wave (Table 3-1).
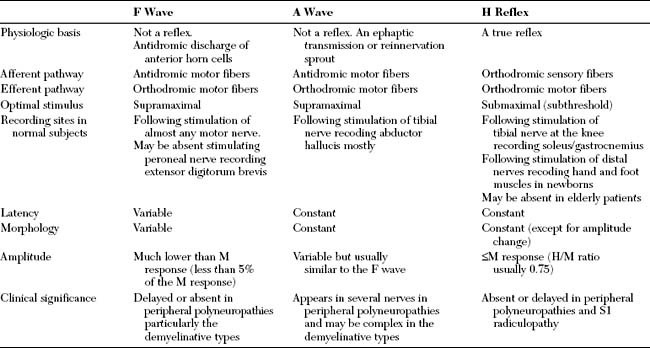
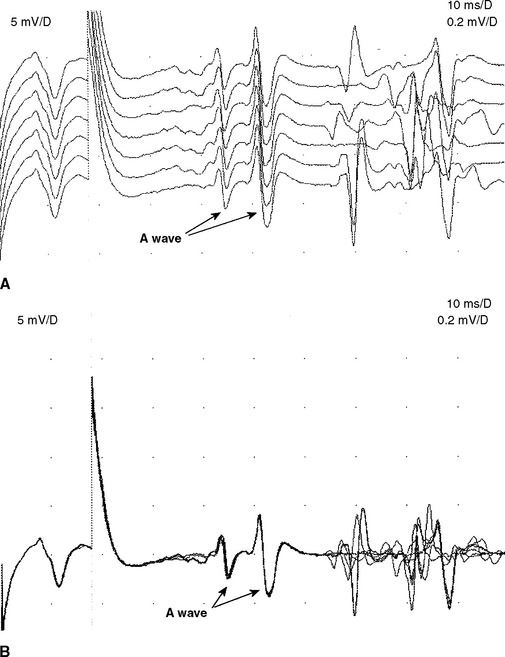
The A wave may be seen in up to 5% of asymptomatic individuals, particularly while studying the tibial nerve (Figure 3-2A and B). In contrast, recording multiple or complex A waves from several nerves is often associated with acquired or inherited demyelinating polyneuropathies (Figure 3-3). A waves are sometimes seen in axon-loss polyneuropathies, motor neuron disease, and radiculopathies. The exact pathway of the A wave is unknown but it may be generated as a result of ephaptic transmission between two axons with the action potential conducting back down the nerve fiber to the muscle. The A wave may also appear following sprouting and reinnervation along the examined nerve. The constant morphology and latency of the A wave is best explained by the fixed point of a collateral sprout or ephapse. When the A wave follows rather than precedes the F response, it suggests that the regenerating collateral fibers are conducting very slowly.
H Reflex
The H reflex, named after Hoffmann for his original description, is an electrical counterpart of the stretch reflex which is elicited by a mechanical tap. Group 1A sensory fibers constitute the afferent arc which monosynaptically or oligosynaptically activate the alpha motor neurons that in turn generate the efferent arc of the reflex through their motor axons. The H reflex amplitude may be occasionally as high as the M amplitude but it is often lower with the H/M amplitude ratio usually not exceeding 0.75.
The H reflex and F wave can be distinguished by increasing stimulus intensity (see Table 3-1). The H reflex is best elicited by a long-duration stimulus which is submaximal to produce an M response, whereas the F wave requires supramaximal stimulus Also, the F wave can be elicited from any limb muscle while the H reflex is most reproducible with stimulating the tibial nerve while recording the soleus muscle which assess the integrity of the S1 arc reflex and is equivalent to the Achilles reflex (Figure 3-4). Finally, the H reflex latency (and often amplitude) is constant when elicited by the same stimulus intensity, since it reflects activation of the same motor neuron pool.
Blink Reflex
The blink reflex generally assesses the facial and trigeminal nerves and their connections within the pons and medulla. It has an afferent limb, mediated by sensory fibers of the supraorbital branch of the ophthalmic division of the trigeminal nerve, and an efferent limb mediated by motor fibers of the facial nerve and its superior motor branches.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


