Chapter 43
Smoking Cessation
A Priority for the Cardiac Patient
1. Why is smoking cessation of fundamental importance in the management of the cardiac patient?
Smoking cessation is the most important of the modifiable risk factors for cardiovascular disease. The products of tobacco smoke contribute directly, and distinctly, to the development of atherosclerosis and the adverse consequences that follow (Box 43-1). The benefits of smoking cessation cannot be exaggerated. A rapid and sustained reduction in the likelihood of cardiac disease or a cardiac event occurs in those who successfully stop smoking; those with established cardiac disease experience a dramatic reduction in the likelihood of recurrence, complication, or death following cessation. In both instances, the benefits of smoking cessation accrue rapidly and reflect the elimination, rather than the ongoing management, of a major risk factor (Table 43-1). Smoking cessation should be accorded a priority in those with cardiac disease—in every professional setting—to do otherwise should be seen as reflective of substandard care.
TABLE 43-1
MORTALITY RISK REDUCTION IN THOSE WITH CORONARY HEART DISEASE
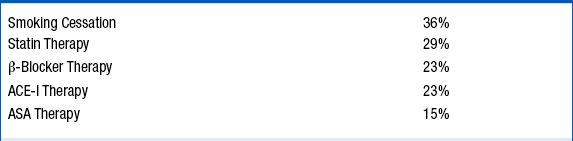
ACE, Angiotensin-converting enzyme; ASA, aspirin.
See: Critchley JA, Capewell S: Mortality risk reduction associated with smoking cessation in patients with coronary heart disease. A systematic review. JAMA 290:86-97, 2003.
2. Why have cardiologists neglected the treatment of tobacco addiction in the past?
3. What should every health care professional know about smoking?
Nicotine is the most addictive substance encountered in ones community. It takes only a few days to establish nicotine addiction once inhalation has been “mastered.” Thereafter, brain function, structure, and neurochemistry become transformed. Smokers smoke to ensure constant levels of nicotine—and the elevated levels of dopamine, and other neurotransmitters, whose release follows the stimulation of nicotine receptors. The cigarette is a perversely engineered drug-delivery device constructed to deliver a precise aliquot of nicotine as rapidly as possible. Following the inhalation of tobacco smoke, nicotine is delivered very rapidly via the arterial system to the brainstem where it initiates a cascade of neurotransmitter activity and dopamine release. Most smokers know why they shouldn’t smoke; most smokers do not want to be smokers; and many smokers will make one or two unassisted quit attempts each year—most of which will fail. Smokers generally do not need more education or lectures. They want help. Optimal cessation strategies involve the following:
 Provision of pharmacotherapy to eliminate or curb the symptoms of withdrawal and craving that lead to the use of a cigarette
Provision of pharmacotherapy to eliminate or curb the symptoms of withdrawal and craving that lead to the use of a cigarette

4. How might smokers with cardiac disease be better assisted with cessation?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


