FIGURE 8-1 Dr. Motomaru Masutani, Dr. Fuminobu Yoshimachi, and Dr. Takashi Matsukage.
What Is Slender Percutaneous Coronary Intervention?
PCI started as an alternative to coronary artery bypass surgery (CABG) in treating coronary artery disease. Despite the long-term superiority of bypass surgery as shown in many comparative studies, the use of PCI has increased over CABG for the last three decades. This is probably due to the less invasive nature of PCI. CABG required general anesthesia, sternotomy, and sometimes cardiac arrest assisted by cardiopulmonary pump. However, PCI required local anesthesia, a small skin incision, and no need for cardiac arrest. It is natural that patients prefer a less invasive strategy.
PCI also has several complications, such as bleeding or embolic complications. Bleeding at the puncture site, such as retroperitoneal bleeding, causes a critical event.1 Even minor bleeding at the puncture site decreases the quality of life of the patient. Although the clinically positive cerebral infarction rate after PCI is reported to be less than 1%, minor cerebral infarction detected by diffusion weight imaging of magnetic resonance after regular PCI was between 10% and 15%.2,3 Cholesterol embolism is a rare complication, but it is critical.4 It may be more frequent in transfemoral intervention (TFI) than in TRI because thick and diffuse atherosclerotic plaques in the descending aorta are the origin of cholesterol embolism in many cases.5 Although it is true that PCI is less invasive than CABG, we need to think of a further less invasive strategy to reduce the complications of PCI. To reduce bleeding complications and cholesterol embolism, the use of a slender guiding catheter in TRI can be an option.
In a narrow sense, “slender PCI” is defined as the use of a smaller device than the routinely used PCI devices. In a broader sense, slender PCI includes all the pursuits of a less invasive strategy of coronary revascularization. Recently launched in Europe by Dr. Ferdinand Kiemeneij and Dr. Shigeru Saito, Slender Club Europe intends to explore new technologies as well as change in practice in order to optimize PCI results. Beyond device miniaturization, this involves risks minimization of any complication, reduction of PCI costs, and same-day discharge.
Device Compatibility in Slender Guiding Catheters
In the early 1990s, balloon angioplasty required 8F guiding catheters. The first Palmaz–Schatz stent was 9F guiding catheter compatible; then its size was reduced to 8F compatible. The first directional coronary atherectomy required a 10F guiding catheter; then there was a gradual downsize to 8F compatible. In the late 1990s, coronary stent size was reduced to 6F guiding compatible. Device compatibility changes all the time, and each size has its own limitations. Thus, we need to choose catheter size according to the required technique for each patient. If access site complication could be ignored, using a bigger catheter might have no technical limitations. However, recent studies have shown that access site bleeding complications relate with worse hard end points; we need to use a guiding catheter as slender as possible. Careful selection of appropriate-size guiding catheter on the basis of the PCI plan for the patient is a modern PCI approach. Specific to radial techniques, slender PCI brings the hope of risk minimization of radial artery occlusion postcatheterization and/or interventions.
New Devices in Slender Percutaneous Coronary Intervention
To achieve slender PCI, we introduce new slender PCI systems.
Downsizing in Regular 0.014 Inch Balloons
Regular 0.014-Inch compatible balloons are getting slender. Previously, the King Ghidorra technique (KGT), that is, simultaneous inflation of three balloons for complex trifurcations, required an 8F guiding catheter. Using new smaller-size balloons, we can do KGT with a 7F guiding catheter.
0.010-Inch Guidewire and Compatible Balloon System
A 0.010-inch wire and compatible balloon system could have a significantly big impact to downsize PCI materials. The 0.010-inch coronary wire system was available at the beginning of the 1990s, but its popularity fell and almost disappeared. Thus, the 0.010-inch system is not new but rather a revival. However, the current 0.010-inch system is smaller than that of the 1990s. The distal tip of some slender balloons is 0.012 inch compatible, that is, smaller than the regular 0.014-inch guidewire. Thus, the passing ability of the device is excellent. Furthermore, the small diameter of those slender balloons made the kissing balloon technique (KBT) possible within a 5F guiding catheter6 and the KGT possible within a 6F guiding catheter.7 With the standard 0.014-inch system, the KBT still requires 6F guiding catheter and the KGT requires 8F guiding catheter.
The IKAzuchi TEN (IKATEN) registry study showed the safety and feasibility of routine use of the 0.010-inch system in the real-world PCI, with a clinical success rate of 99%.8 The passing ability of the balloon was also excellent. However, the 0.010-inch guidewire did not allow stents to pass a bended lesion due to less supporting ability. Despite this, the 0.010-inch guidewire had a high success rate in passing through chronic total occlusion (CTO), a fact supported by Masutani et al.,9 who reported the efficacy of the 0.010-inch system for CTO lesions.
The Prospective multicenter registry of IKAzuchi-X for CHronic total occlUsion (PIKACHU) registry study10 was then conducted to show the efficacy of the 0.010-inch system for CTO lesions. About 68% of lesions were successfully treated only with 0.010-inch system from the antegrade approach, whereas 86% of lesions were successfully treated using any devices including the 0.014-inch system. The 68% success rate was notable only from the antegrade approach. Recently, we have started the G-FORCE study, which is a multicenter prospective randomized trial, to show the superiority of the guidewire having a distal tip size of 0.010 inch or less for the CTO treatment. This study intends to show the superiority of using slender guidewires for CTO lesions.
Small-Size Intravascular Ultrasound Catheter
In a 5F guiding catheter, it is impossible to use the Atlantis pro-intravascular ultrasound (IVUS) catheter (Boston Scientific, Marlborough, MA) with a 0.014-inch guidewire. However, it is possible if the guidewire is 0.010 inch. Interestingly, two 0.010-inch guidewires can be passed through the Atlantis pro-IVUS catheter, even though a single 0.014-inch guidewire cannot. On the contrary, the Eagle eye IVUS catheter (Volcano, San Diego, CA) can be used with a 0.014-inch guidewire. Boston Scientific has recently launched a new version of its IVUS catheter which is now compatible with 5F guiding catheters.
The View-it IVUS catheter (Terumo) can also be used with a 0.014-inch guidewire in a 5F guiding catheter. Thus, some Japanese IVUS-oriented PCI operators turned to slender PCI because the View-it system has the same ability as the Atlantis IVUS catheter. The View-it IVUS system is available only in Japan. IVUS guide parallel wire technique for complex CTO PCI requires an 8F guiding catheter. However, it can be downsized to a 7F using the View-it IVUS catheter.
New Techniques in Slender Percutaneous Coronary Intervention
Bifurcation Treatment in Slender Percutaneous Coronary Intervention
Bifurcation lesions remain a challenge in today’s PCI11 (see Chapter 18). Crush stenting requires an 8F guiding catheter because two stents should be inserted in a guiding catheter (Table 8-1). The crush stent technique is simple and easy. However, it is not widely performed currently because of low long-term patency at the side branch.12,13 If we do not perform the crush technique, we can reduce the guiding catheter size. Except for the backup problems, device compatibility is similar between 6F and 7F in bifurcation treatment. As it is impossible to perform KBT in a 5F guiding catheter without a 0.010-inch system,6 it has been a limitation of 5F for bifurcation lesions. The clinical impact of KBT is more debatable now, but many operators still use it routinely. As far as KBT is concerned, the 0.010-inch system has great impact on the bifurcation treatment.6 Then, left main bifurcation can be treated in TRI14 even using 5F.6 Furthermore, the KGT is now possible within a 6F guiding catheter using the 0.010-inch system.7
Chronic Total Occlusion
Many operators treat CTO lesions in TRI.15 However, it requires strong backup force to pass a balloon or a microcatheter into the CTO lesion. Thus, many operators prefer larger guiding catheter to treat CTO. Some easy CTO lesions such as those with no calcification, short lesions, and straight lesions with low J-CTO score16 can be treated using a 5F catheter. Some operators are interested in a 5F guiding catheter for retrograde approach because a microcatheter passage like corsair is enough for the retrograde catheter. At present, a 5F guiding catheter has many limitations in treating CTO (e.g., impossible parallel wire technique).
TABLE 8-1 Bifurcation Treatment Technique
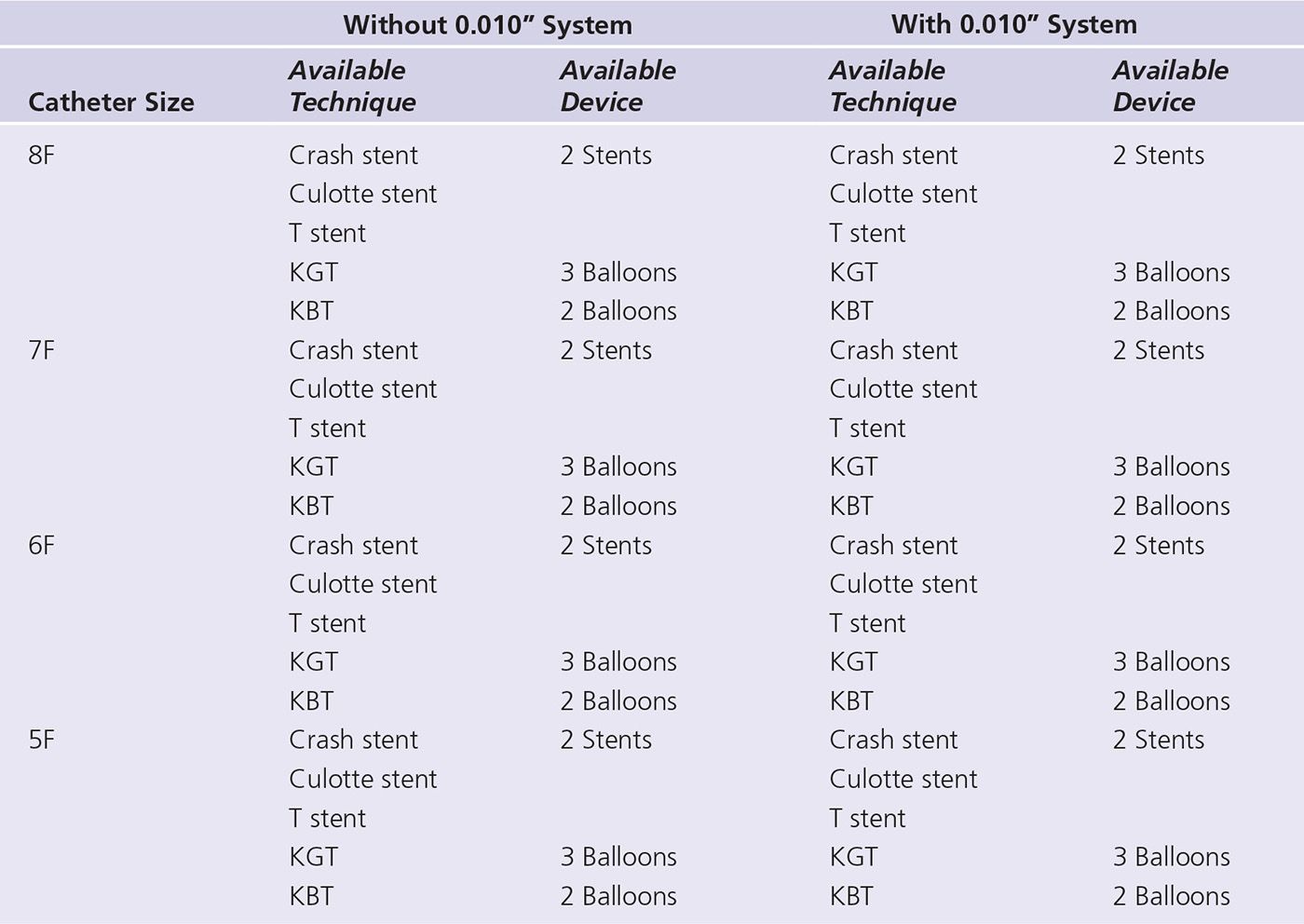
KGT, King Ghidorra technique; KBT, kissing balloon technique.
Masutani et al.9
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


