1. Primary snoring
2. Upper airway resistance syndrome (UARS)
3. Obstructive sleep apnea/obstructive sleep hypopnea syndrome (OSAHS)
4. Central sleep apnea
5. Asthma
6. Chronic obstructive pulmonary disease (COPD).
partner is bothered by the snoring and is experiencing sleep difficulties themselves. The focus in treatment is based on whether the patient has daytime symptoms and other features associated with SDB. A thorough history should include a review of risk factors associated with primary snoring. Known risk factors are listed in Table 2.2.
TABLE 2.1 Essential Elements of the Sleep History for Sleep Disordered Breathing | ||
|---|---|---|
|
TABLE 2.2 Risk Factors for Primary Snoring | |
|---|---|
|
Unrefreshing sleep
Excessive daytime sleepiness
Poor or reduced performance
Headaches
Difficulty concentrating or attentional deficits.
has an abnormal airway anatomy, he or she may need additional evaluation for possible surgical intervention.
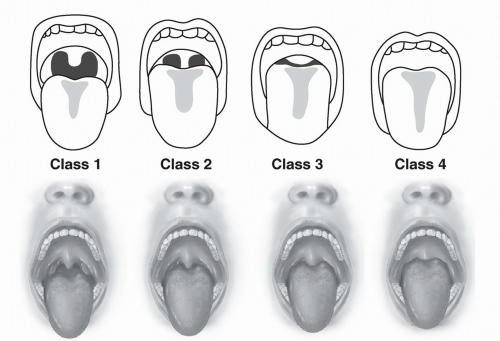 FIGURE 2.1 The Mallampati classification describes tongue size relative to oropharyngeal size. The test is conducted with the patient in the sitting position, the head held in a neutral position, the mouth wide open and relaxed, and the tongue protruding to the maximum. The subsequent classification is assigned based upon the pharyngeal structures that are visible. Class I = visualization of the soft palate, fauces, uvula, anterior and posterior pillars; Class II = visualization of the soft palate, fauces, and uvula; Class III = visualization of the soft palate and the base of the uvula; Class IV = soft palate is not visible at all. If the patient phonates, this falsely improves the view. If the patient arches his or her tongue, the uvula is falsely obscured. The test was initially adapted to predict ease of intubation but can be used to predict the potential severity of obstructive sleep apnea (OSA). (See references 7 and 8.) (Modified after Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J 1985;32:429-434.) |
Asymptomatic snorers contemplating a surgical treatment for snoring
Asymptomatic snorers with known vascular disease, including hypertension
Asymptomatic snorers, as they may have UARS or OSAHS.
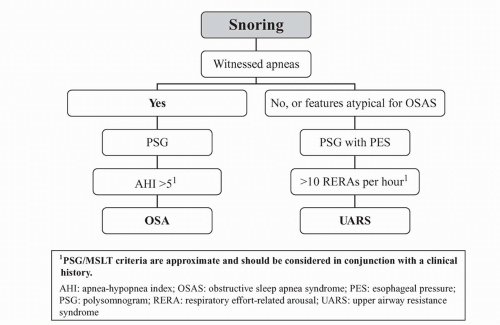 FIGURE 2.2 Algorithm for the evaluation of snoring. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


