Fig. 14.1
(a) Triangular leaflet resection repair: The area of segmental prolapse is identified. The triangular resection includes the prolapsing posterior leaflet with the triangle “point” extending to the valve annulus; (b) Triangular leaflet resection repair: After completing the triangular resection, the leaflet defect is repaired with interrupted polypropylene sutures; (c) Triangular leaflet resection repair: A flexible annuloplasty band is then implanted with braided 2–0 suture, beginning at the right fibrous trigone, continuing clockwise, using a running suture technique; (d) Triangular leaflet resection repair: After running suture from the right trigone to the mid-annulus, a second suture is started at the left fibrous trigone and advanced to the center of the band and tied to complete the implantation
Limited Resection with In-Folding Leaflet Plasty
If a larger leaflet segment must be resected, we perform a limited quadrangular resection (Fig. 14.2a) and cross sutures from the middle of each leaflet edge to the annulus (Fig. 14.2b). By tying both sutures, adjacent leaflet edges are folded onto the annulus (Fig. 14.2c). The residual defect is closed using a running suture with a limited leaflet sliding-plasty (Fig. 14.2d). The repair is completed by implantation of an annuloplasty band as described previously.
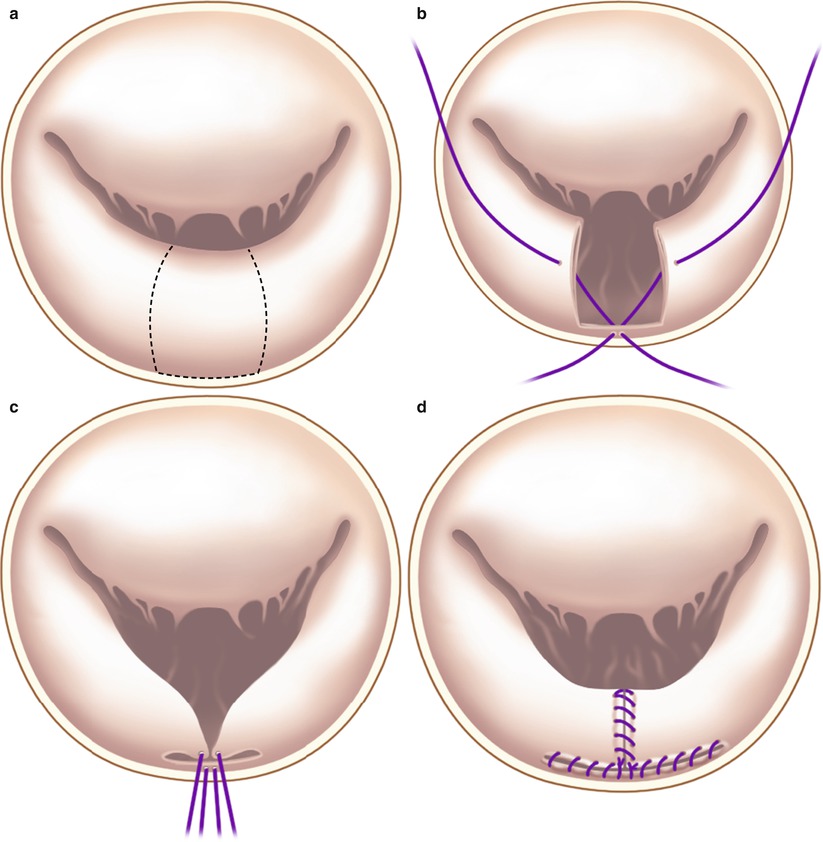
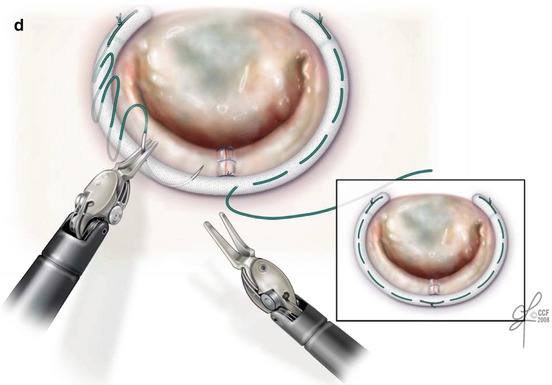
Fig. 14.2




Folding-plasty leaflet repair (a) When the prolapsed area is broad and the leaflet segment is tall, the segment is removed as in a classic quadrangular resection. (b) Sutures are taken through the mid-portions of the leaflet remnants, crossed, and passed through the annulus. (c) Tightening sutures to the annulus reduces leaflet height. (d) The leaflet remnants are sutured to each other and to the annulus, completing the leaflet repair. The repair is followed by insertion of an annuloplasty band as described earlier
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
