Shift-Work Sleep Disorder: Sleep and Performance in Medical Training
Shift-Work Sleep Disorder: Sleep and Performance in Medical Training
Valentina Gumenyuk
Christopher L. Drake
SHIFT-WORK DISORDER
Shift-work is now a major element of 24/7 working life across a broad range of industries and services, including medical, transportation, and communication. A significant number of workers are engaged in “nonstandard” working hours, including shift work (morning, afternoon, night- and rotating-shift systems), weekend work, compressed work week, seasonal work, and extended work (on-call). Improved “efficiency” and “safety” are a major concern for shift work systems in the U.S. and other countries. The demands of the shift-work system can impact the well-being, performance, and sleep of shift workers through a variety of factors. The majority of night shift workers (60%-70%) complain about their sleep; specifically, difficulties falling and staying asleep, poor quality of sleep, short sleep duration, and difficulties staying awake during working hours (1). Partially due to these adverse effects a number of devastating incidents, such as Bhopal, Three Mile Island, Chernobyl, the Rhine chemical spillage, and the Exxon Valdez oil spill have occurred. These incidents are examples of why shift work requires more attention and action toward safety and health issues.
This chapter reviews the current state of knowledge of one major clinical factor, shift-work disorder, associated with sleep-wake disturbances and their impact on human functioning. The relation of extended work hours to sleep and cognitive ability in medical training will be also addressed.
SHIFT-WORK SCHEDULE
In the United States, more than 21 million wage and salary workers (17.7%) work atypical work hours that fall at least partially outside the typical daytime (from 8 AM to 6 PM) work–shift range. The most common is an evening shift, with normal hours between 2 PM and midnight, accounting for 6.8% of workers. These workers usually have late bedtimes and an absence of napping (2).
Some workers of the morning shift (from about 5 AM to about 2 PM) may show a sleep pattern more disturbed as compared to night shift workers (3). In addition, those on morning shift experience short total sleep time as night workers do (4). The main complaint is early awakening and feelings of non-refreshing (5). This feeling can be associated with reduced slow wave sleep (the marker of homeostatic processes), as measured by electroencephalography (EEG) (6). The nature of this shift is associated with early time of rising (between 4 AM and 5 AM) and is strongly associated with increased sleepiness during the rest of the day (7). Th at is why the vast majority of morning-shift workers nap in the early afternoon (2,8) as well as right after a morning shift (9).
The work hours between 9 PM and 8 AM correspond to night shifts (3.1%), and periodically changing work hours correspond to rotating shifts (2.7%) (10). Most studies and research reports refer to shift work that includes night work, since this is recognized to be a serious risk factor to workers’ health and safety. Night shift is frequently (30%-50%) associated with napping in the afternoon before work, especially if the preceding sleep time has been reduced (11). Night workers have significantly reduced total sleep time by 2 to 4 hours (4,12). Often, to compensate for their short total sleep time, night workers nap before and during their work shift. Thus, about one-third of night-shift workers use a late afternoon nap (duration greater than one hour) that varies between individuals and depends on the length of the preceding sleep loss (13). This type of work is characterized by increased subjective and objective sleepiness (see below for more details) (14,15)5. The eff ect of maximal sleep pressure may occur in the early morning, often involving involuntary sleep episodes while attempting to remain awake. This severe increased sleepiness may be related to an increased risk of accidents (16,17), which are discussed later in this chapter.
DIAGNOSTIC EVALUATION
The more severe sleep-wake problems are recognized as a diagnostic hallmark of shift-work disorder (SWD) in the International Classification of Sleep Disorders (American Academy of Sleep Medicine, 2005). The diagnostic criteria of SWD are:
complaint of insomnia or excessive sleepiness associated with a work schedule;
symptoms directly associated with the shift-work schedule during the course of at least 1 month;
circadian and sleep-time misalignment, as demonstrated by sleep log or actigraphic monitoring for 7 days or more;
sleep disturbance not explainable by another sleep disorder or by a medical, neurological, or mental disorder; medication use; or substance-use disorder.
Potential factors that may trigger shift-work disorder are: vulnerability to insomnia (17), genetic predisposition to sleep loss (18) and to circadian variation (19), and age (20).
ADVERSE EFFECTS ON HEALTH OF SHIFT WORKERS
The adverse effects on health of working shifts are well documented (21, 22 and 23). They include disruption of physiological processes, including the sleep-wake cycle (24); the impairment of physical and psychological health (25); problems with alertness, performance, and safety (5,26); and interference with social and personal life (27). Long-term shift workers are also reported to have a higher incidence of some types of cancers compared to dayworkers, particularly breast cancer in female shift workers (28,29). A possible relationship between shift work and breast cancer was first identified in 1987 by Stevens, who proposed that the suppression of melatonin by light during night-shift work might lead to an increased risk of breast cancer, though this mechanism has not been proven.
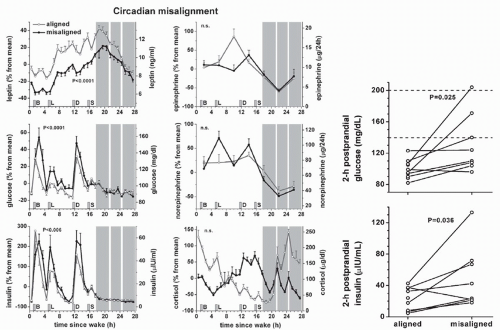
There is also evidence that sleep debt impacts the immune (30) and endocrine systems (31). Scheer et al. (32) at Harvard Medical School maintained 10 healthy subjects on an artificially long sleep-wake cycle. After 10 days, the investigators evaluated metabolic, autonomic, and endocrine function. As shown below, subjects displayed significantly altered metabolic measures. Overall, glucose was 6% higher and insulin was 22% higher during circadian misalignment when compared with the state of circadian alignment. Additionally, several individuals displayed prediabetic or diabetic postprandial glucose levels when circadian rhythms were misaligned but not prior to misalignment (Fig. 20.1). These data suggest that abnormally aligned sleep-wake cycles may contribute, in select patient populations, to the development of a prediabetic or diabetic state. Finally, mean arterial blood pressure was significantly increased by 3% in subjects with circadian misalignment, an elevation shown previously to be significantly associated with increased risk of morbidity and mortality (33,34).
FIGURE 20.1 Illustration of metabolic measures during circadian mis(alignment) across 10 healthy subjects. This result also does suggest that the acute adverse cardiometabolic consequences observed in patients with impaired sleep may be due to circadian misalignment. (From Scheer FA, Hilton MF, Mantzoros CS, et al. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc Natl Acad Sci U S A 2009;106(11):4453-4458, with permission.)
In a large epidemiologic sample (2,570 individuals) Drake et al. (17) observed the prevalence and consequences of SWD. Significant differences were found on a variety of measures between workers who met criteria for SWD as compared to nonsymptomatic shift workers (Table 20.1). Thus, the greater morbidity was found in individuals with SWD than in workers without SWD. In terms of risk, the odds ratio for ulcers in night workers with SWD was 3.82 (95% confidence interval [CI] = 1.18-12.32), and the odds ratio for ulcers in rotating workers with SWD was 4.30 (95% CI = 1.67-11.09) relative to shift workers without SWD. For the combined group of shift workers with SWD, the odds ratio for ulcers was 4.18 (95% CI = 2.00-8.72) (see Table 20.1).
While all these negative effects on health are very significant, the most common complaints among night and rotating shift workers are sleep disturbances that reduce alertness and performance and increase the rate of accidents (35, 36, 37, 38 and 39). About 75% of workers leave shift work due to difficulties and problems from trying to cope with atypical hours for sleep and work (40,41). The irresistible biological need for sleep is necessary for maintaining wakefulness upon the trough of the alertness rhythm. In individuals with high sleep pressure (due to sleep disturbances or sleep loss), involuntary sleep can happen while they are in the workplace or while driving home, which can be more dangerous than the impact of sleep deprivation on health.
MECHANISMS OF SLEEP AND WAKE REGULATION
The sleep-wake cycle is regulated by two separate but interacting mechanisms: the homeostatic and circadian processes (42.43). The function of the homeostatic process is regulation of sleep debt. Sleep debt increases during wakefulness and decreases during sleep. The homeostatic system is presumably located in the anterior region of the hypothalamus (44) and is modulated in the brain by physiologic, biochemical, and molecular processes that build up only during wakefulness and decline during sleep. The nature of this process remains unclear (45). A circadian process can be described as a nearly 24-hour internal oscillatory variation of the sleep-wake cycle and consolidation of sleep-wake behavior by opposing the increase in sleep drive (homeostatic) associated with sustained wakefulness (46).
The circadian pacemaker (master clock) is located in the suprachiasmatic nuclei (SCN) of the hypothalamus. The master clock is composed of thousands of oscillator neurons of the hypothalamus, each dependent on the cell-autonomous actions of a defined set of circadian clock genes. Still, the major question remains how these individual oscillators are organized into a biological clock to produce a coherent output that is able to time all the different daily changes in our behavior and physiology. However, it is well known that the SCN seems to contain neurons that specifically target the liver, pineal and adrenal glands, and coordinate our day-night functions and behavior (47). The SCN neurons have a genetically determined rhythmic activity that is modulated by light. These clock genes have been associated with diurnal preferences, providing an explanation of why some of us feel more alert relative to others during “morning” or “evening” hours.
The human sleep-wake cycle is not simply driven by the SCN, rather there is a complex interaction between components of the system that generate circadian rhythmicity and sleep homeostasis. The circadian variation in sleep propensity is closely associated with the circadian rhythm of body temperature and melatonin. Melatonin is often referred to as “hormone of darkness” because it is secreted in the absence of light. The normal pattern (rhythm) of melatonin secretion is that levels rise approximately 2 hours prior to bedtime (9:00 PM), then reach a peak during the early hours of the morning (at about 4:00 AM), and then fall again. Melatonin has effects via specific receptors and SCN appear to be rich in these receptors. The pineal gland produces and secretes melatonin. Whereas the pituitary gland and retina in addition to the liver, kidney, heart, and epithelium may be influenced by the circadian clock, because they contain melatonin receptors (48). Shift work disturbs the circadian rhythm by regularly requiring sleep at adverse circadian phases (i.e., daytime), which can lead to both sleep disturbances and impaired daytime functioning (49,50).
TABLE 20.1 Mean ± Standard Deviation of Morbidity and Sleep Measures in Shift Workers Who Met or Did Not Meet Criteria for Shift-Work Disorder and Day Workers With and Without Symptoms of Insomnia or Excessive Sleepiness
aSignificant difference between individuals meeting criteria for shift-work disorder (SWD) and those who did not meet criteria (main effect of SWD was only tested if the omnibus-F value or Chi-Square was significant); depression was determined using the Diagnostic Interview Schedule based on the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV) criteria; for missed work as well as missed family and social activities, the number of days refers days missed during the past 3 months.
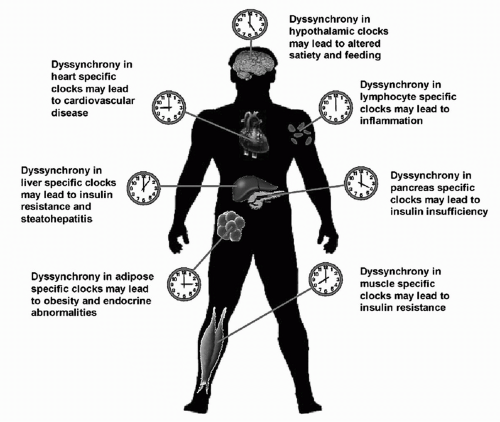
FIGURE 20.2 Schematic illustration of dyssynchrony of peripheral circadian clocks potentially leading to the pathogenesis of multiple facets of cardiometabolic disorders. (From Young ME, Bray MS. Potential role for peripheral circadian clock dyssynchrony in the pathogenesis of cardiovascular dysfunction. Sleep Med 2007;8(6):656-667, with permission.)
Young and Bray (51) illustrated (Fig. 20.2) the desynchronization of the peripheral circadian clock that potentially may contribute to the pathogenesis of the cardiometabolic system. Disruption of normal synchronization between skeletal muscle, adipose tissue, liver, hypothalamus, and pancreas likely accelerates insulin resistance, insulin insufficiency, and dyslipidemia, the hallmarks of cardiometabolic syndrome associated with circadian misalignment. Disruption of circadian clocks within the heart and vasculature may accelerate cardiovascular disease.
There are also associations between polymorphisms in the gene CLOCK (activity of this gene favors sleep), obesity, and metabolism. A particular mutation of this gene can increase the risk for metabolic syndrome and obesity (52).
DESYNCHRONIZED CIRCADIAN PHASE IN SHIFT-WORK DISORDER
In shift-work, exposure to the complex combination of environmental zeitgebers (time cues; e.g., light) can promote a shift of circadian phase. The term “circadian phase” describes the internal time location during a 360-degree cycle, usually the peak or trough of the cycle with reference to some external point, such as local time or habitual sleep time. The core body temperature at the minimal level (nadir) and dimlight melatonin onset (DLMO) are commonly used as measures of circadian phase. A circadian phase shift can either advance or delay the body clock, and it appears that light is regarded as the most beneficial modulator of this shift (53). This was demonstrated in simulated (laboratory) night-shift studies (53, 54, 55, 56, 57 and 58), as well as in field night-work studies (59, 60 and 61). Partial adaptation by phase advance occurs in some permanent hospital night workers; for example, after two to five night shifts, the phase (evaluated by melatonin measures) in night workers showed an advance as compared to control (day-working subjects) (62). In the isolated work conditions of the Antarctic, adjustment to night shifts is seasonally dependent. Midwinter and Arendt (63) demonstrated a phase shift greater than 9 hours during summertime (continuous environmental light) and more than 5 hours during winter (continuous environmental dark) relative to the day-working subjects.
Due to this phase shift, some long-term night-shift workers may experience an increased risk of health problems and safety since their internal biological rhythms are out of phase with their sleep-wake schedule. Also, they may have an individual predisposition for SWD and/or other medical problems.
There are robust interindividual differences, with some patients remaining at their normal diurnal phase position while others delay or advance their circadian timing in response to night work. The nature of this difference is not clear. One of the substantial sources of this variation might be the morningness-eveningness interindividual difference (64). Other possible reasons for the differences in circadian pacemaker response to shift-work include age-related differences (65,66)
Only gold members can continue reading. Log In or Register to continue