FIGURE 20-1 Radial artery size in 250 Japanese patients. (From Saito S, Ikei H, Hosokawa G, et al. Influence of the ratio between radial artery inner diameter and sheath outer diameter on radial artery flow after transradial coronary intervention. Catheter Cardiovasc Interv. 1999;46:173–178.)
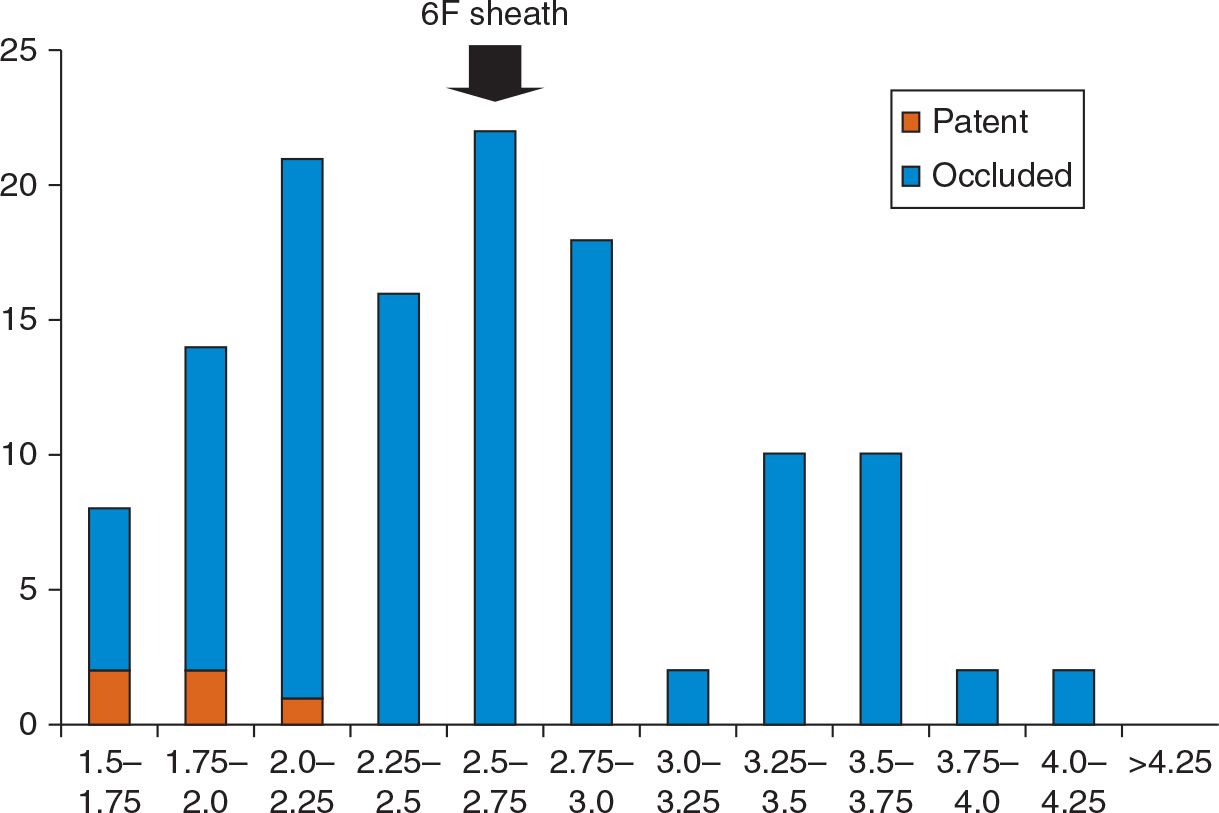
FIGURE 20-2 Radial artery size distribution and associated radial patency postprocedure in 124 Caucasian patients.
The Asahi Eaucath has a central dilator tapered onto a 0.035-inch wire that both straightens the curved catheter shape and has smooth transitions from the wire to the catheter (Fig. 20-4). The catheter is also hydrophilically coated to allow atraumatic insertion. As the dilator is tapered onto a 0.035-inch wire, usual practice is to insert a 4F or 5F sheath, advance a 0.035-inch wire, and then remove the sheath, leaving only the wire in situ. Following advancement into the aorta, the dilator is removed, and the guide springs back into a range of popular shapes for coronary cannulation and behaves similar to a conventional guide catheter. Catheters may be exchanged over a 0.035-inch wire directly into the radial artery. The proximal end of the catheter may be fixed in position using an adhesive dressing during PCI.
The performance of these catheters has been reported in several studies. Following the European launch in 2007, we were the first to report the use of sheathless guide catheters. We described the use of the 7.5F sheathless in 17 patients undergoing complex PCI with the use of bifurcation techniques or adjunctive equipment requiring a larger bore size than 6F.19 Procedural success using a sheathless guide was achieved in all cases. Several subsequent studies have similarly shown that 7.5F sheathless guides are well tolerated for complex interventional procedures requiring a large-bore guiding catheter.20 Following this in 2010, we reported the use of the 6.5F sheathless guide in 100 patients undergoing routine PCI.21 Procedural success was 100%, and there were no catheter-related complications reported. Casemix included 25% patients undergoing primary PCI and 50 patients undergoing urgent PCI for ACS, and procedures included a range of adjunctive equipment and techniques compatible with 6F. Radial occlusion was observed in only two patients. Our conclusion was that sheathless guides could completely replace conventional guiding catheters for both routine and complex PCI. Recently, a very large series of 7,853 procedures has confirmed the utility and safety of these devices that were used in 76% of all PCI procedures by 43 operators over an 8-year period at a single Japanese center.22 Procedural success using sheathless guides was very high (98.9%), with a low catheter-induced coronary osteum dissection rate (0.2%).
TABLE 20-1 Proportion of Patients in Whom the Radial Lumen Is Less Than the Diameter of Conventional 4F, 5F, 6F, and 7F Sheaths
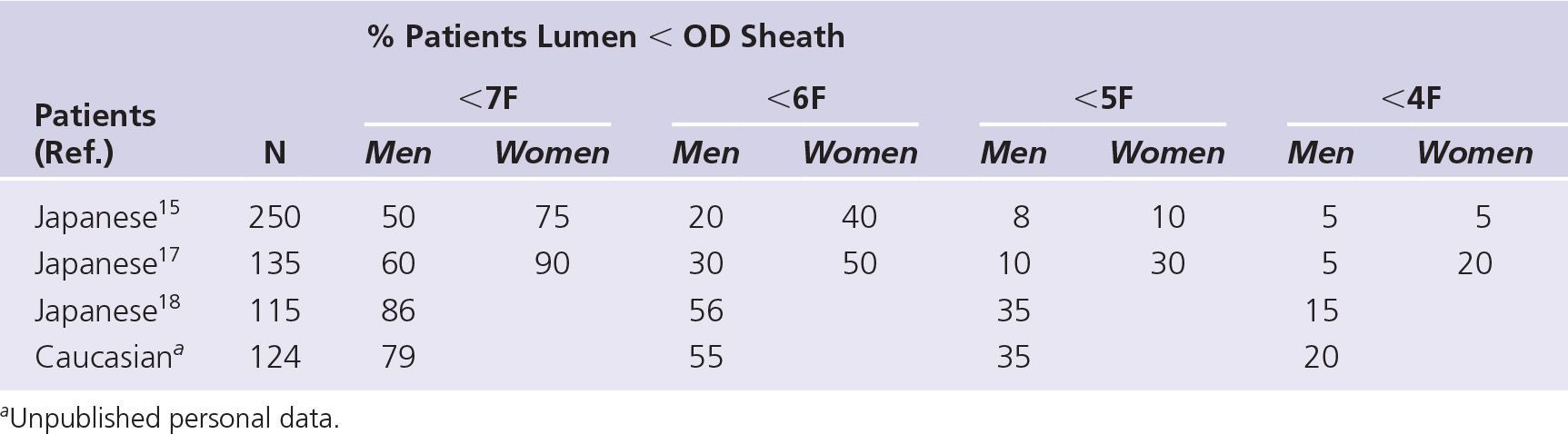
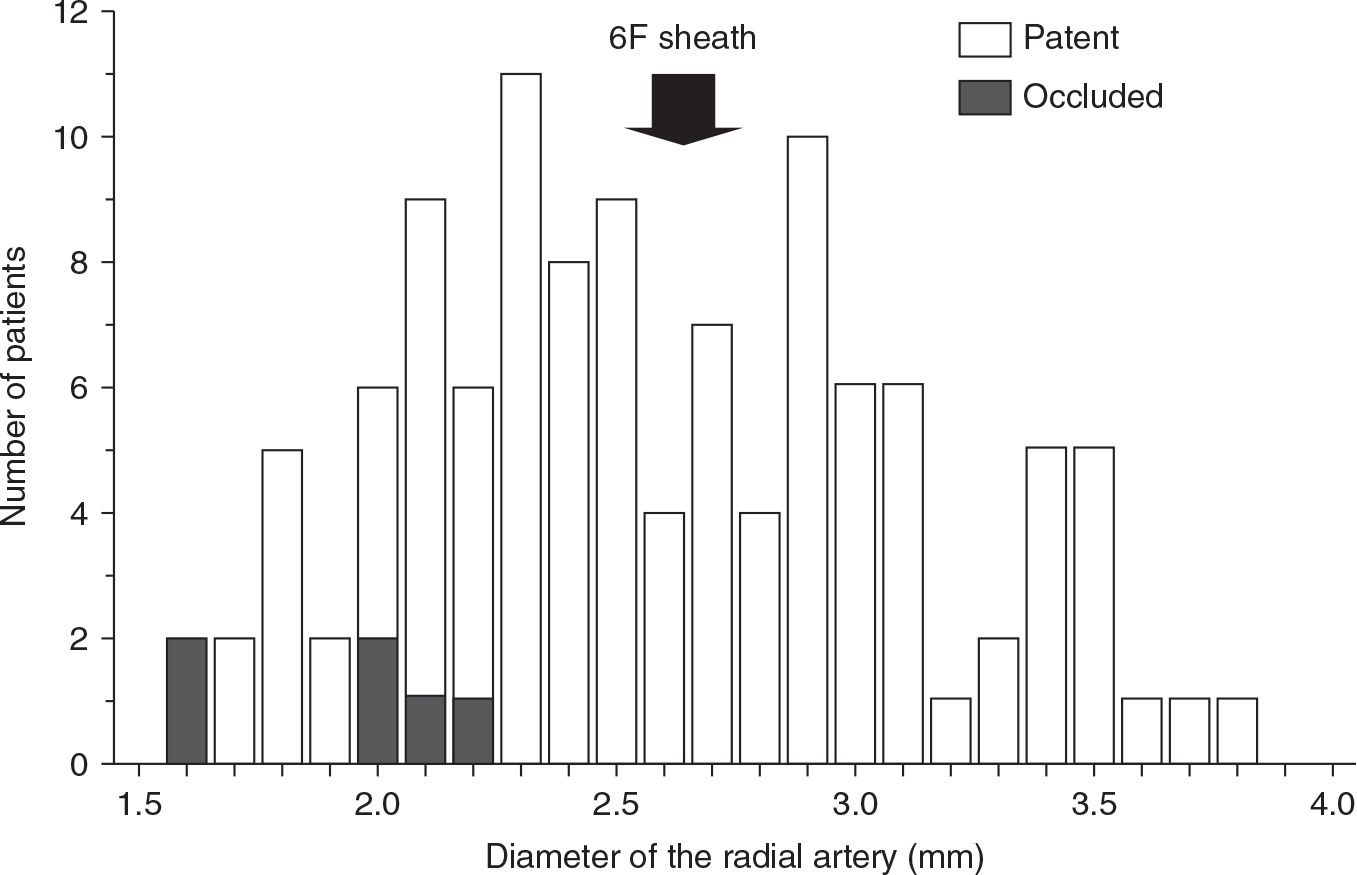
FIGURE 20-3 Radial artery size distribution and associated radial patency post procedure in 115 Japanese patients. (From Kwan TW, Cherukuri S, Huang Y, et al. Feasibility and safety of 7F sheathless guiding catheter during transradial coronary intervention. Catheter Cardiovasc Interv. 2012;80:274–280.)
We have subsequently compared two consecutive cohorts of patients (unpublished data). In the first sheathless cohort of 231 patients, transradial intervention (TRI) was performed using sheathless guides in 212/213 patients and crossover to conventional guide due to catheter tip dissection in one patient. In the second conventional cohort of 304 patients, TRI was performed using conventional sheaths in 271/285 patients, with crossover to sheathless due to small radial artery in 14 patients. Greater pain was associated with the use of 7F conventional sheaths than with the sheathless 7.5F; however, pain scores for 6F compared to 6.5F sheathless were similar. Radial occlusion rates were also similar at 4.4% using conventional and 3.7% using sheathless guides at 2 months.

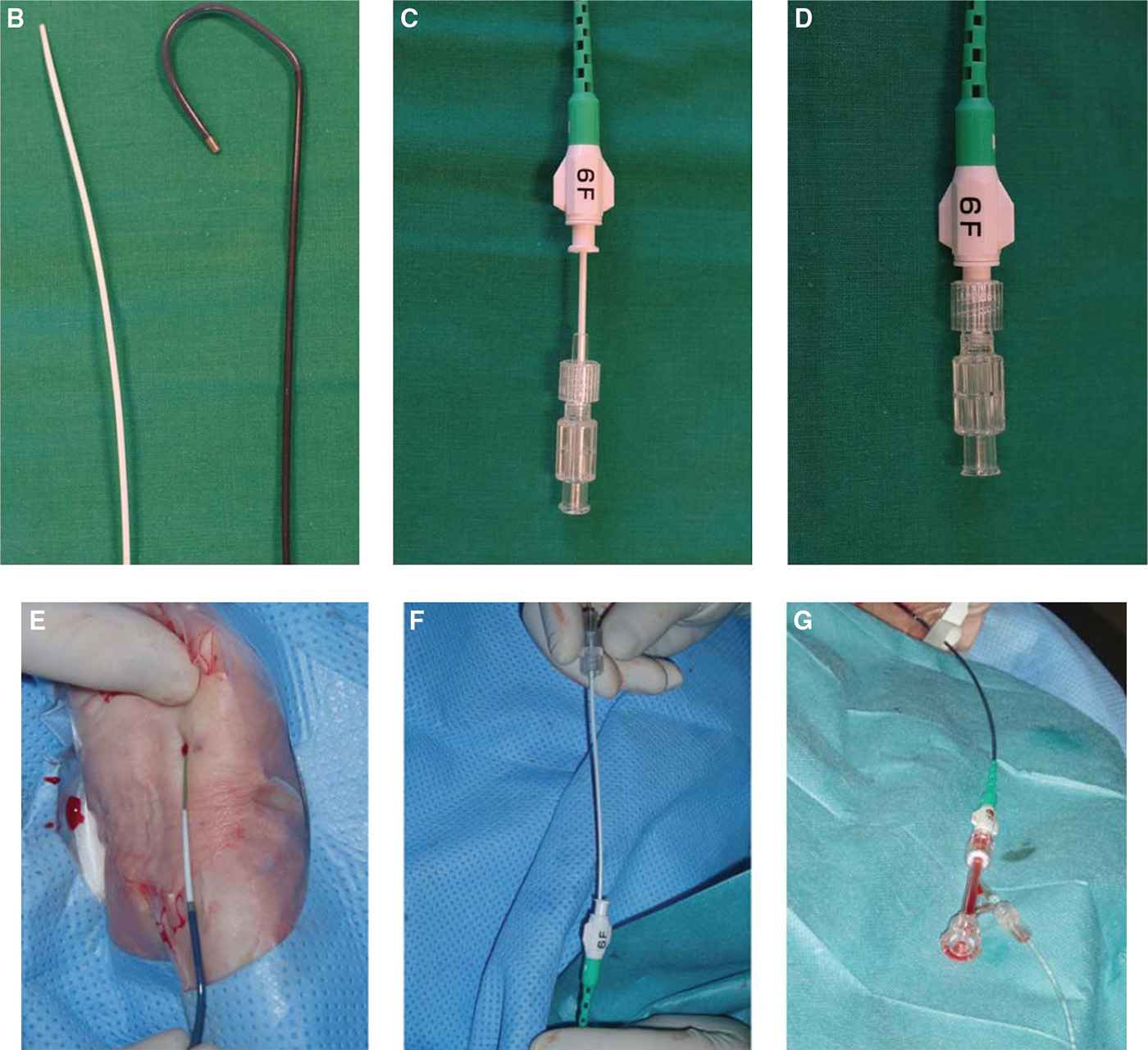
FIGURE 20-4 Method of sheathless guide insertion. A: Prior insertion of a 4F or 5F sheath used for prior angiography if required and for insertion of a 0.035-inch wire. B: Eaucath with its dilator. C: Dilator inserted into Eaucath. D: Dilator fixed at distal end of Eaucath. E: Eaucath advanced over a 0.035-inch wire and dilator into radial artery (after removal of sheath). F: Dilator removed when catheter in aorta. G: Proximal end connected to Y connector.
These studies, therefore, show that while Asahi sheathless guides are a very effective and safe alternative to conventional guides, the lower profile of equipment has not yet been shown to translate into reduced radial pain and injury. Further studies are needed to investigate the reasons. Furthermore, as the catheters are stiffer than conventional guides and lack the support and functionality of a sheath, they are somewhat more cumbersome to use. The need for insertion over a 0.035-inch wire as well as prior angiography in ad hoc PCI also necessitate the prior insertion of a 4F or 5F sheath, negating some of the benefits of a sheathless system. It is difficult therefore to fully endorse the routine use of Asahi sheathless guides.
However, the selective use of sheathless guides can be fully supported. Radial artery size varies widely, and can be approximated by palpation or measured directly using ultrasound. The 6.5F sheathless guide is a good option for patients with small radial arteries, frequent in women, in whom it is likely to be much better tolerated than a 6F sheath while allowing a greater range of interventional options than 5F. Similarly, for patients with small and average-size radial arteries, 7F conventional sheaths are often poorly tolerated and 7.5F sheathless guides are a good option. Such selective use has been reported in several studies, showing very high procedural success.16,20,23 Sciahbasi et al.20 reported a procedural success of 100% in 79 patients with small radial arteries and 134 patients with potentially complex bifurcation transradial PCI using 6.5F and 7.5F sheathless guides, respectively. Similarly, Youn et al.23 reported a 100% procedural success for non-CTO (chronic total occlusion) lesions in 29 patients with very small radial arteries that were all smaller than a 5F sheath (<2.3 mm) and had a mean diameter of only 1.8 mm. The 6.5F sheathless guides are particularly suited to us in small radial arteries because not only is the diameter significantly smaller than that of a 5F sheath (2.16 compared to 2.3 mm), but also the catheter is hydrophilic along its length, and the presence of the central dilator smoothes the transitions and eliminates the “razor effect” caused by the gap between the catheter and the wire.24
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


