Cardiac injuries due to penetration by sharp foreign bodies usually have a clear clinical presentation. A case of a 38-year-old man with self-inserted cardiac lesions and a misleading presentation is reported. The patient was admitted to the emergency room because of chest pain, with increase in biomarkers of myocardial necrosis, and electrocardiographic and echocardiographic abnormalities inducing initial diagnostic and therapeutic workup of acute coronary syndrome. Once clinical destabilization followed by death had occurred, the suspicion of an alternative diagnosis came from delayed chest radiography, confirmed by autopsy, revealing the presence of multiple metallic objects within the thorax.
Cardiac injuries produced by sharp penetrating foreign bodies (sewing needles, acupuncture needles, fragments of Kirschner wires, and bullets) may occur both accidentally, either in adults or in children, and after acupuncture therapy, domestic violence, or as a result of self-inflicted injury due to abuse of opioids or mental disorders, herein representing a suicide attempt. Clinical presentation of cardiac injuries by foreign bodies is usually clear. We report a case of a patient admitted to the emergency department with an initial suspicion of acute coronary syndrome and an unexpected final postmortem diagnosis.
Case Report
A 38-year-old male Romanian inmate was admitted to the Emergency Room of the Pisa Hospital, Italy, because of chest discomfort and dyspnea, occurring while in jail. The patient was agitated and not collaborative, thus making medical interview difficult. At admission, physical examination showed sinus tachycardia (heart rate 122 beats/min), normal oxygen saturation (98%), fine crackles at lung auscultation, and an anterior chest scar suggesting previous sternotomy. Electrocardiogram revealed Q waves in inferior leads and inverted T waves in the precordial leads; biomarkers of myocardial necrosis were found to be slightly increased (troponin-T 0.27 ng/ml, upper reference limit 0.14, CK-MB 16 ng/ml, upper reference limit 6.3). An echoscopic study revealed normal size and global left ventricular function (left ventricular ejection fraction 58%), inferior wall hypokinesis, no significant valve dysfunction, and mild pericardial effusion with fibrin clots stratified on the posterior wall. An acute coronary syndrome was therefore initially suspected, and treatment with nitrates, aspirin, β blockers, and oxygen was initiated, but a brisk deterioration of the clinical status occurred with hypotension, oxygen desaturation, and sinus bradycardia, followed by loss of consciousness. Cardiopulmonary resuscitation maneuvers were initiated ineffectively, with subsequent death of the patient. Once clinical destabilization followed by death had occurred, the suspicion of an alternative diagnosis came from delayed chest radiography report, revealing the presence of multiple metallic objects within the left anterior chest and hypochondrium.
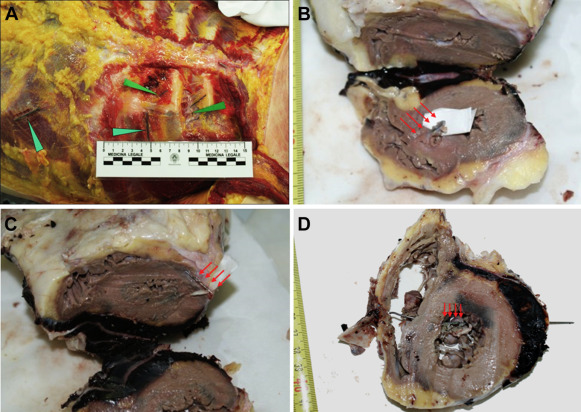
A forensic autopsy was requested to clarify the cause of death. The external examination of the body showed the median sternotomy scar of the previous open-heart intervention; some acupuncture signs were evident in precordial region. After anatomic dissection, 5 needles were found embedded out of the thorax in the precordial region ( Figure 1 ), and 3 more at the base of the left costal arch under the subcutaneous fat. Two needles were detected in the abdomen. A small area of hemorrhagic infiltration was present to the left sternal border ( Figure 1 ). Once thorax was opened, a relevant mediastinum hematoma with about 500 cm 3 of fluid and clotted blood were discovered. At section of the heart, 2 further smaller metallic objects were found (one partially embedded in the apex, another one entirely infixed in the left ventricular anterior-lateral; Figure 1 ). A sharp metallic object, 9-cm long, impaled in progression in the anterior face of the pericardium, right ventricular free wall, interventricular septum, left- ventricular lateral wall, and inferiolateral pericardium ( Figure 1 ). The pierced myocardial areas were bruised. Likely because of previous adhesive pericarditis, hemopericardium was present only in the posterior region ( Figure 1 ). Eleven metallic objects are shown in Figure 2 .