8 Role of Echocardiography in Patients Treated with Cardiotoxic Drugs
Basic Principles
• Agents most commonly associated with cardiotoxic risk include anthracyclines (doxorubicin), as well as the tyrosine kinase inhibitors trastuzumab, sunitinib, and sorafenib (Table 8-1).
• Cardiotoxicity associated with anti-cancer therapy is typically associated with a global decline in left ventricular ejection fraction (LVEF), although early manifestations may include diastolic dysfunction.
• Echocardiography is important to assess both systolic and diastolic cardiac function, extent of valvular disease, and evidence for any pericardial disease.
TABLE 8-1 COMMON CHEMOTHERAPY AND ANTI-CANCER AGENTS ASSOCIATED WITH SIGNIFICANT CARDIOTOXICITY
| Type of Agent | Potential Cardiac Complication |
|---|---|
| Anthracyclines | |
| Doxorubicin | Early postinfusion, transient, often reversible decline in LVEF; arrhythmias, myopericarditis; more commonly, a decline in LVEF > 1 year after therapy |
| Tyrosine Kinase Inhibitors | |
| Trastuzumab | Potentially reversible, significant decline in LVEF |
| Bevacizumab | Hypertension, arterial thrombosis |
| Sunitinib | Decline in LVEF, hypertension |
| Sorafenib | Myocardial infarction, hypertension |
| Imatinib | Diastolic dysfunction, pericardial effusion |
| Alkylating Agents | |
| Cisplatin | Hypertension, vascular dysfunction |
| Cyclophosphamide | Pericarditis/myocarditis, decline in LVEF with high doses |
| Antimetabolites | |
| 5-Fluorouracil | Coronary vasospasm, myocardial ischemia |
| Antimicrotubules | |
| Paclitaxel | Arrhythmia, heart failure |
Anthracycline Cardiotoxicity
• Doxorubicin cardiotoxicity can occur early or late during therapy. Early changes occur acutely or within the first year of therapy. Late dysfunction occurs months or many years after the initial exposure.
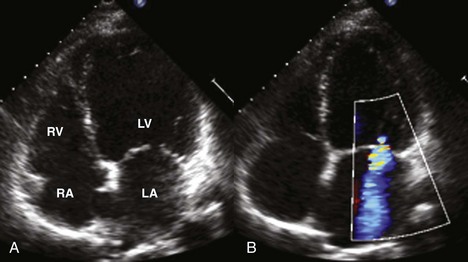
• Overall, doxorubicin cardiotoxicity is indistinguishable from other forms of heart failure with LV dilatation, wall thinning, and decreased contractility (Figure 8-1).
• An increased risk of cardiotoxicity is associated with higher cumulative dosages of doxorubicin (particularly > 550 mg/m2) and with pre-existing cardiac disease, including hypertension, valvular disease, and ischemic heart disease.
Trastuzumab Cardiotoxicity
• Cardiotoxicity risk is increased in the setting of prior exposure to anthracyclines as well as concomitant cardiovascular disease such as hypertension or coronary disease.
• Cardiotoxicity is often observed during the treatment phase and can be reversible with cessation of therapy or institution of cardioprotective medications.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


