Fig. 31.1
A TEE study shows outflow obstruction because of ventricular septal hypertrophy combined with systolic anterior motion of the mitral valve anterior leaflet (SAM)
Operative Technique
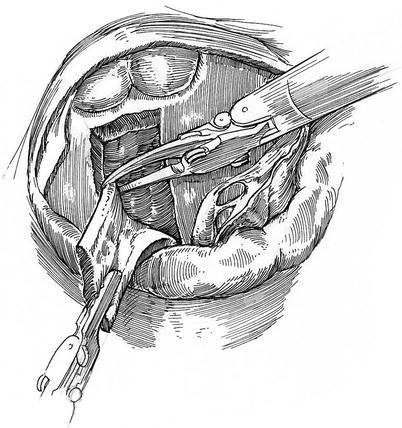
After the left atriotomy is made, the mitral valve anterior leaflet attachment (aorta-mitral curtain) is exposed using the dynamic robotic retractor. The left fibrous trigone is defined and from here the anterior leaflet incised, carrying the incision toward the left fibrous trigone. At least 2-mm of anterior leaflet remnant must remain to facilitate leaflet reattachment (Fig. 31.2). Then the divided anterior leaflet falls away and into the left atrium, revealing the bowing hypertrophied ventricular septum and anterior papillary muscle (Fig. 31.3). Generally, the right fibrous trigone/anterior leaflet attachment can be left as a marker for reconstruction. Frequently, the anterior leaflet is elongated as much as 3-cm or more. Often a ridge exists across the long anterior leaflet, indicating the site coaptation with the posterior leaflet and the distal leaflet bowing toward the ventricular septum. This is an important finding as the distance from this fibrous ridge to the anterior leaflet tip is the length that it should be shortened during re-attachment.
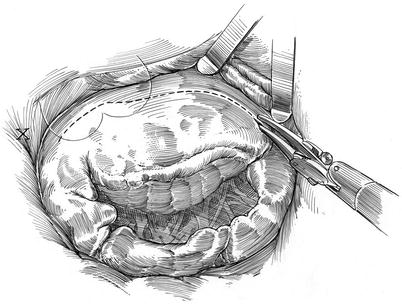
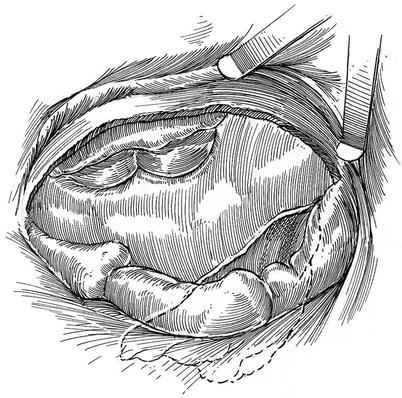
Fig. 31.2
The anterior leaflet is detached from the left fibrous trigone proceeding clockwise toward the right fibrous trigone. At least 2 mm of residual anterior leaflet should be preserved to afford leaflet reattachment
Fig. 31.3
Detachment of the anterior leaflet provides excellent exposure of the hypertrophied inter-ventricular septum. The origin of the aortic valve cusps is defined by antegrade cardioplegia delivery
We start the septal myectomy with curved robotic scissors, beginning near the left fibrous trigone, which is now oriented somewhat leftward and posterior (Fig. 31.4). This is in contradistinction to the traditional trans-aortic view, which reveals the septum to be resected somewhat anterior. Extreme care must be taken to avoid injury to the aortic valve leaflets. Administration of antegrade cardioplegia helps to identify the base of aortic valve leaflets. The resection then is carried in a clockwise direction toward the nadir of the right coronary aortic valve leaflet. A generous section of septum is removed, based on TEE measurements. Often a subvalvular fibrous ridge exists and must be excised carefully. An overzealous resection past the mid-septum can eventuate in conduction system injury. Following a generous septal resection, the anterior papillary muscle is freed to the base of all septal attachments, so that it becomes mobile, allowing full excursion of the anterior leaflet and chords (Fig. 31.5).