Fig. 19.1
Leaflet prolapse with annular calcium – An islet of annular calcium is shown along with a flail posterior leaflet P2 segment due to ruptured chordae tendenae. Using robotic Resano forceps and a heavy needle holder the calcium is being dislodged, softening the native mitral annulus
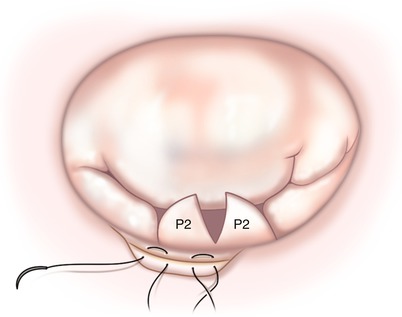
Fig. 19.2
Leaflet resection and annular reconstruction. A conservative triangular leaflet resection of P2 has included the ruptured chord segment. The debrided annulus is being reconstructed using horizontal mattress sutures
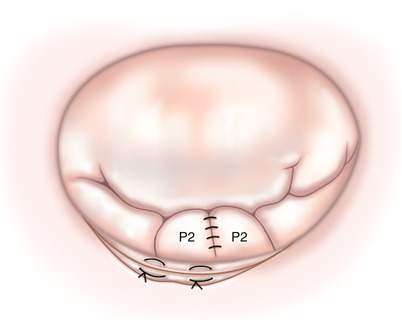
Fig. 19.3
Leaflet and annular repair. The triangular leaflet defect has been closed using interrupted monofilament sutures. Annular reconstruction suture have been tied
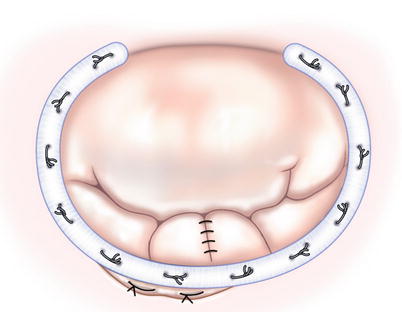
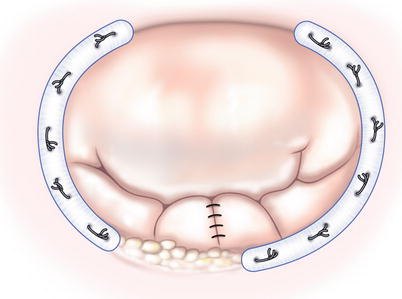
Fig. 19.4
Annuloplasty band insertion. Using interrupted mattress sutures an annuloplasty band has been deployed from mitral valve trigone to trigone using horizontal mattress sutures. The band not only reduces the annular size, allowing better leaflet coaptation, but also supports the annular reconstruction
For an isolated extensively calcified area of the posterior annulus, debridement may not be prudent, especially if calcium extends into the ventricular wall or onto the leaflet. In this circumstance, usually do a standard leaflet repair and then attach the annuloplasty band to the right fibrous trigone, suturing it clockwise until the calcium is addressed. Then, the band is divided and suture attachment is restarted on the other side of the calcified islet (Fig. 19.5). Band anchoring is continued to the left fibrous trigone. Although the band does not circumscribe the annulus completely, sufficient distraction occurs between posterior scallop edges against the anterior leaflet to obtain adequate coaptation, resolving the leak. We have had no annular “break downs” using this technique and no recurrent regurgitation secondary to annular dilatation in this limited area.