Fig. 26.1
Incision and robotic instrument placement: after determining the aortic valve level from the preoperative CT scan, the working-port incision is made directly over the corresponding interspace. The robotic endoscopic camera is placed through the medial aspect of the incision. Thereafter instrument trocars are passed under camera visualization into the thorax via the 2nd intercostal space (ICS) [left arm] and 5th ICS [right arm]. The aortic cross-clamp is passed through the chest wall at the axillary 4th ICS
The ascending aorta is cross-clamped using a trans-thoracic aortic cross clamp inserted previously through the axillary chest wall. An aortic root infusion of cold crystalloid cardioplegia is given to affect cardiac asystole and myocardial protection. Thereafter, the aorta is retracted toward the incision with sutures. Throughout the arrest period, the pericardial well is irrigated with saline. To maintain a clear operative field, a left ventricular vent is positioned through the right superior pulmonary vein.
After a transverse aortotomy has been made, we place three commissural sutures to retract and expose the aortic valve annulus. Robotic scissors and forceps are inserted through the pre-placed trocars. Then, the surgical cart of daVinci™ Surgical System (Intuitive Surgical Inc., Sunnyvale, CA) is docked to these instruments, and the aortic valve is excised (Fig. 26.2). Any calcific debris is removed by irrigation and suction. Using a robotic needle holder, we place 12 subannular pledgeted 2/0 Ethibond sutures (Ethicon, Somerville, NJ) around the annulus (Fig. 26.3). Care is taken to arrange sutures in an organized fashion around the incision. Suture guides are helpful for this purpose (Fig. 26.4). Thereafter, sutures are passed through the sewing ring of the prosthesis, which then is seated at the annulus (Fig. 26.5). All knots are tied by the tableside assistant and secured in place with a knot pusher. De-airing is done through a vent placed in the ascending aorta and is facilitated by filling the ventricle and ventilating.
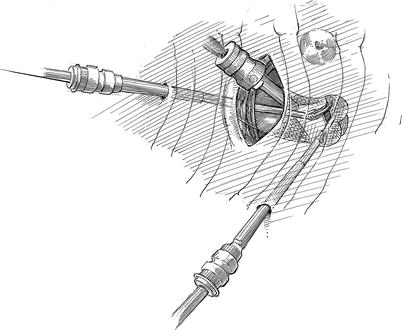
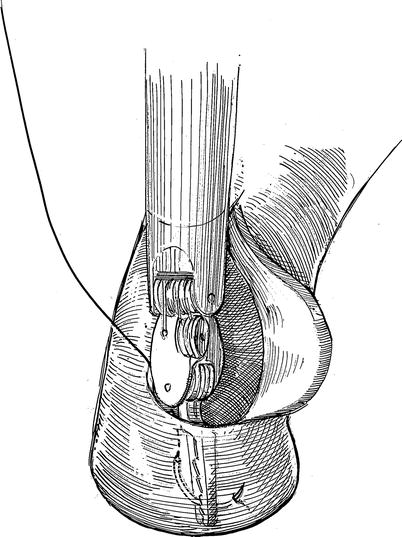
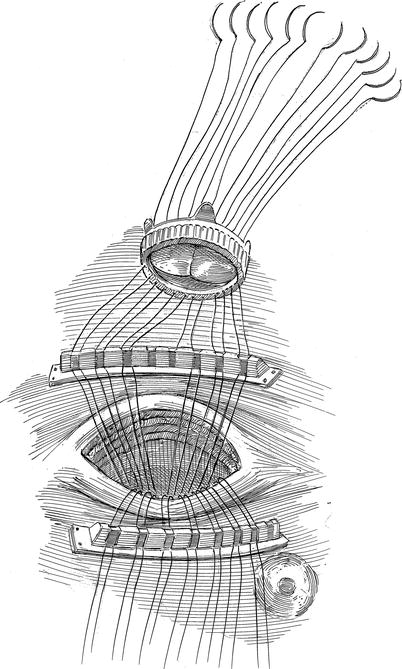
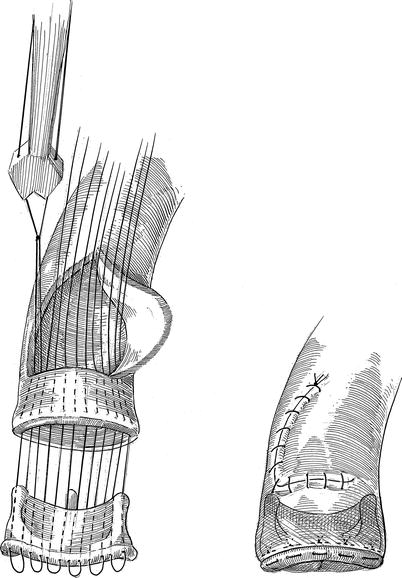
Fig. 26.2
Robotic instruments in place and excising the aortic valve—a transverse aortotomy is made using the curved robotic scissors. Then, the diseased aortic valve is excised. Calcium can be debrided using large needle holders
Fig. 26.3
Annular suture placement: after valve excision and debridement, subannular 2-0 braided sutures are placed robotically around the annulus and retrieved through the working incision
Fig. 26.4
Suture organization and sewing ring placement: as sutures are brought through the working incision, they are arranged around the incision. Suture guides can facilitate and maintain suture organization. Then, the tableside surgeon passes each suture through the prosthetic valve sewing ring. Thereafter, the prosthesis is lowered to the native aortic annulus
Fig. 26.5
Prosthetic valve implantation—knot tying: after the prosthetic valve has been seated at the native annulus and any redundant suture loops tightened, each knot is tied and secured by the tableside assistant using a knot pusher
Tips and Pitfalls
Adequate visualization of the aortic valve is the most important aspect of the robotic valve replacement. The thoracic incision must be made close to the region of the aortic valve. This is either in the third or fourth ICS, depending on the anatomic location as determined by the pre-operative CT scan.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


