INDICATIONS AND CONTRAINDICATIONS
Resection of a mainstem bronchus with pulmonary preservation is indicated when the disease process is limited to the mainstem bronchus only. The first documented bronchial sleeve resection was performed by Price Thomas in 1947 for a carcinoid tumor located in the right mainstem bronchus. A circumferential resection was performed with primary anastomosis, and thus the patient was able to maintain functional use of both lungs postoperatively and survived long term. Frequently, it is low-grade malignant bronchial tumors and very rare benign neoplasms that account for centrally located lesions arising in the mainstem bronchus. Since a minimal bronchial margin is usually required for clearance and cure of these neoplasms, pneumonectomy is very rarely necessary to perform an adequate oncologic resection. Mainstem bronchoplastic procedures, as described in this chapter, allow for removal of the lesion or tumor with conservation of any uninvolved lung parenchyma, thereby yielding the best functional result for the patient (Fig. 39.1).
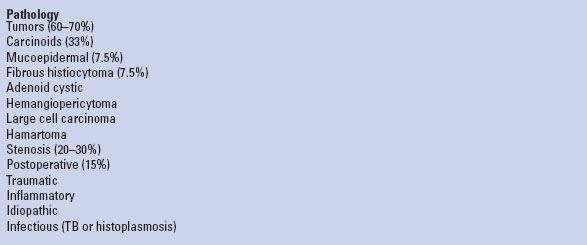
The most common diseases requiring mainstem bronchial sleeve resection are relatively rare low-grade or benign airway neoplasms, including carcinoids, mucoepidermoid tumors, adenoid cystic carcinomas, fibrous histiocytomas, hemangiopericytoma, and hamartomas. Less common benign lesions include isolated mainstem bronchial stenosis secondary to granulomatous disease, that is, tuberculosis, trauma, or foreign body. Mainstem disruption from blunt or penetrating traumatic injury has also been described. Nonsmall cell bronchogenic carcinomas are quite rare and make up only approximately 2% of mainstem lesions. In two published series from the Massachusetts General Hospital, left mainstem resections appear to be twice as common as right mainstem resections, which may reflect disease predilection, as well as more likely, anatomic considerations such as amenability to resection and length of the mainstem bronchus (Table 39.1).
There are no true absolute contraindications for mainstem bronchoplasty per se. Relative contraindications of mainstem resection apply to all bronchoplastic procedures, and there are three primarily to consider: (1) Active bronchial inflammation, (2) high-dose corticosteroids, and (3) high-dose radiation more than 1 year prior to resection. Active inflammation of the airway, especially in the setting of tuberculosis, at the point of reconstruction has a high likelihood of resulting in postoperative bronchial stenosis. As bronchoplastic procedures tend to be performed under greater tension, in the instance where the patient is undergoing therapy with corticosteroids, it is advisable to buttress the reconstruction with a material more substantial than pleura, that is, pedicled pericardial fat, omentum, or intercostal muscle. Lung transplantation is certainly an example where a bronchial anastomosis is performed routinely in patients on high-dose steroids, but generally not under tension. A history of high-dose radiation to the chest or mediastinum in excess of 5,000 cGy more than 1 year prior to bronchoplasty carries an extraordinarily high risk of dehiscence. The higher the dose and more remote the timing of previous irradiation, the greater the risks associated with bronchoplasty. If undertaken, these reconstructions are most reliably buttressed with an omental flap pedicled on the right gastroepiploic arcade.
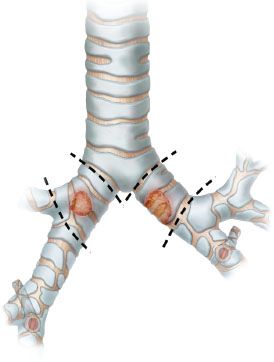
Figure 39.1 Lesions of the mainstem bronchus.
Postobstructive pneumonia does not represent a contraindication to sleeve resection, provided that the lung parenchyma is still salvageable. Lung parenchyma that is chronically atelectatic can be re-expanded and regain useful function. Intravenous antibiotic therapy, serial therapeutic aspiration bronchoscopy at the bedside, and possible prebronchoplasty endobronchial core-out to relieve obstruction are all measures that may serve to optimize lung function and clear infection. Aggressive clearance of any pus and secretions in the airway distal to the obstruction is critical.
TABLE 39.1 Pathology of Mainstem Bronchial Lesions
 PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
Bronchoscopy, both flexible and rigid, is the single most important component of the preoperative evaluation for sleeve resection to identify and biopsy any endobronchial disease limited to main bronchus, and also to determine the extent of diseased area, and its amenability to resection and reconstruction. It should generally be performed at the time of initial evaluation and diagnosis, as well as immediately prior to any bronchoplastic procedure to assess the quality of the mucosa in terms of active airway inflammation and secretions.
To undergo mainstem bronchoplasty, patients must be cleared from a medical standpoint for open posterolateral thoracotomy. Furthermore, pulmonary function testing and quantitative ventilation–perfusion scanning should be done routinely to evaluate cardiopulmonary reserve. Pneumonectomy is always a possibility during these procedures for either expected or unexpected reasons, ranging from adequacy of oncologic resection to technical complications, and postpneumonectomy pulmonary function needs to be specifically calculated in advance to assess whether it can be tolerated.
In the case of malignant neoplasms, assessment of regional nodal involvement and metastatic disease should be undertaken using computerized tomography with intravenous contrast, if possible, and positron emission tomography, though some of these lesions may demonstrate varying degrees of FDG uptake. Radiologic evaluation via spiral CT or virtual bronchoscopy can also be helpful in revealing tumor size, location, and extent of disease globally. Mediastinoscopy may be indicated to confirm nodal involvement, though not routinely. In addition, mediastinoscopy may be a useful technique to facilitate anterior dissection of the pretracheal planes down to the level of the carina.
 SURGICAL TECHNIQUE
SURGICAL TECHNIQUE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


