Rib Destruction
Christopher M. Walker, MD
DIFFERENTIAL DIAGNOSIS
Common
Metastases
Multiple Myeloma
Bronchogenic Carcinoma
Less Common
Osteomyelitis
Ewing Sarcoma
Rare but Important
Chondrosarcoma
Osteosarcoma
Askin Tumor
Empyema Necessitatis
Langerhans Cell Histiocytosis
Lymphoma
Other Sarcomas
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Age of patient
≤ 30 years old
Ewing sarcoma
Askin tumor
Langerhans cell histiocytosis
Osteosarcoma
≥ 40 years old
Metastatic disease
Multiple myeloma
Bronchogenic carcinoma
Differentiate from benign causes that may expand ribs but do not destroy cortex
Fibrous dysplasia, enchondroma, brown tumor
Helpful Clues for Common Diagnoses
Metastases
Most common cause of rib destruction in adults
Ribs contain red marrow so highly vascular
Polyostotic (multiple lesions)
History of primary tumor
Most common tumors to metastasize to rib are breast, lung, kidney, or thyroid carcinoma
Most common solitary rib metastasis secondary to thyroid or renal cell carcinoma
Multiple Myeloma
2nd most common cause of rib destruction in adults
Most common bone manifestation is generalized osteopenia
Solitary expansile lytic lesion may indicate solitary plasmacytoma
Biopsy required for definitive diagnosis
Bronchogenic Carcinoma
Rib destruction secondary to Pancoast tumor or hematogenous metastases
Pancoast tumor
Syndrome of ipsilateral arm pain, Horner syndrome, and ipsilateral hand muscle wasting
Superior sulcus tumor invades apical fat to involve brachial plexus and sympathetic ganglia
Rib destruction is best sign to definitively diagnose chest wall invasion
MR occasionally used to assess for neurovascular invasion
Helpful Clues for Less Common Diagnoses
Osteomyelitis
May be difficult to distinguish from Ewing sarcoma or Askin tumor
Aggressive lytic lesion with wide zone of transition
± soft tissue mass
Usually occurs in association with empyema, pneumonia, or chest wall infection
Chronic osteomyelitis
± periosteal reaction
± sclerosis of involved ribs
Ewing Sarcoma
5-15% arise in ribs
Adolescents and young adults usually present with painful chest wall mass
Small round blue cell tumor
Radiographic patterns
80% are lytic with bone destruction
10% are mixed lytic/blastic lesions
10% are sclerotic
40% have expanded rib
Most have disproportionately large soft tissue mass compared to osseous involvement
Intrathoracic component ≥ extrathoracic component
Metastasizes most commonly to bone
Epicenter on rib
Heterogeneity of mass reflects tumor necrosis
Bone scintigraphy demonstrates increased activity in affected rib and helps diagnose metastatic disease
Helpful Clues for Rare Diagnoses
Chondrosarcoma
Patient 30-60 years old ± chest wall pain
Occurs anteriorly or near costochondral junction
Radiographs and CECT show
Large mass with bone destruction
± soft tissue involvement
Chondroid matrix (rings and arcs calcification)
Osteosarcoma
Patient 10-30 years old with painful mass
Bone destruction secondary to heterogeneous soft tissue mass
± cloud-like osteoid matrix
Lung is most common site of metastatic disease
Metastases may calcify
Askin Tumor
Form of primitive neuroectodermal tumor (PNET)
Arises in soft tissues of thorax
Children and young adults present with chest wall pain
Radiographs show
Heterogeneous mass ± rib destruction
Rib destruction less common than Ewing sarcoma
± pleural effusion
Metastasizes to lung and bone
Empyema Necessitatis
Empyema that subsequently invades through chest wall
Most common related bony abnormality
Rib sclerosis or periosteal reaction secondary to chronic osteomyelitis
Organisms can be remembered by BATMAN pneumonic as BATMAN breaks through barriers
Blastomyces
Actinomyces
Tuberculosis (75% of cases)
Mucor
Aspergillus
Nocardia
Langerhans Cell Histiocytosis
Expansile lytic lesion
No sclerotic rim
Polyostotic
± soft tissue mass
Lymphoma
Heterogeneous or homogeneous soft tissue mass
± mediastinal lymphadenopathy
Extrathoracic disease is common
30% have lung involvement
Peaks in 5th-8th decades of life
Other Sarcomas
Rib destruction seen with
Rhabdomyosarcoma, malignant fibrous histiocytoma, and synovial sarcoma
Image Gallery
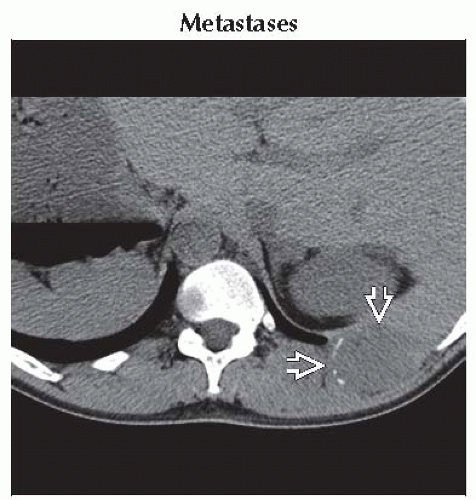 Axial NECT shows an expansile lytic rib lesion with large soft tissue component  . Lower sections (not shown) revealed a heterogeneous mass in the kidney in this patient with proven renal cell carcinoma. . Lower sections (not shown) revealed a heterogeneous mass in the kidney in this patient with proven renal cell carcinoma. |
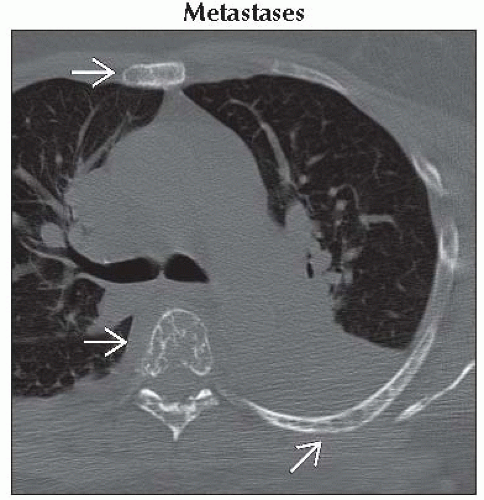 Axial NECT shows multiple lytic bone lesions within the ribs, vertebral body, and sternum  . This patient had a history of breast cancer and was experiencing bone pain. . This patient had a history of breast cancer and was experiencing bone pain. |
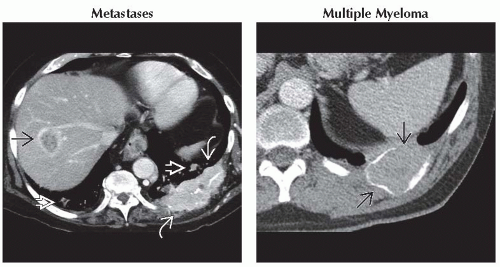 (Left) Axial CECT shows a large enhancing soft tissue mass destroying a left posterior rib
 . Note ring-enhancing hypervascular liver metastasis . Note ring-enhancing hypervascular liver metastasis  with central low density. There are also lung metastases with central low density. There are also lung metastases  in this patient with metastatic renal cell carcinoma. (Right) Axial CECT shows an expansile soft tissue mass involving a posterior rib in this patient with metastatic renal cell carcinoma. (Right) Axial CECT shows an expansile soft tissue mass involving a posterior rib  . This proved to be a solitary plasmacytoma on biopsy. . This proved to be a solitary plasmacytoma on biopsy.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|