Although heparin administration has reduced the incidence of radial artery occlusion (RAO) during the transradial coronary angiography (TRCA), the effective activated clotting time (ACT) value for guiding unfractionated heparin dosing in patients undergoing TRCA is unknown. Four hundred thirty-two patients who were scheduled for elective TRCA were enrolled in our prospective study. All the patients received a standard dose of 5,000 IU unfractionated heparin. Anticoagulation level was assessed by ACT measurements that were taken at the end of the procedure just before the sheath removal. The day after TRCA, all patients were evaluated by color Doppler ultrasound to detect RAO. RAO was found in 29 patients (6.7%). A median ACT of 205 seconds in the RAO group and 265 seconds in the radial artery patent group were detected (p <0.001). Mean procedure duration was significantly longer in the RAO group than in the radial artery patent group (18.55 ± 9.80 vs 11.24 ± 7.07 minutes, p <0.001). There was a negative correlation between end-procedural ACT and procedure duration ( r = −0.117, p = 0.015). In multivariate analysis, end-procedural ACT (odds ratio 0.981, 95% confidence interval [CI] 0.972 to 0.989, p <0.001), procedure duration (odds ratio 1.076, 95% CI, 1.037 to 1.116, p <0.001), and radial artery diameter (odds ratio 0.240, 95% CI 0.063 to 0.907, p = 0.035) were found as independent predictors of RAO. In conclusion, shorter end-procedural ACT levels, longer procedural duration, and smaller radial arterial diameter were independently associated with RAOs after TRCA with standard-dose heparin. In prolonged procedures, ACT-based heparin dosing may be useful to overcome RAO.
Since the first introduction of transradial access for coronary angiography, it has gained popularity because of the less access site complications, less bleeding, and shorter hospital stay. In contrast, the major postprocedural drawback of transradial coronary angiography (TRCA) is radial artery occlusion (RAO) that encounters in 1% to 10% of cases. Fortunately, systemic anticoagulant agents decrease the risk of RAO after transradial interventions. In contrast to coronary angioplasty in which weight-adjusted unfractionated heparin (UFH) is used, for diagnostic TRCA, a standard nonadopted dose of UFH is recommended. Activated clotting time (ACT) described by Hattersley in 1966 is used to monitor the level of anticoagulation with heparin in patients undergoing percutaneous coronary intervention and cardiopulmonary bypass surgery, and ACT level is shown to be correlated with hemorrhagic complications. Whether end-procedural ACT is related to RAO that is a thrombotic process in the TRCA remains unclear. The aim of this study was to evaluate the relation between RAO rate and end-procedural anticoagulation level represented by ACT after a standard dose of 5,000 IU UFH in patients undergoing elective TRCA.
Methods
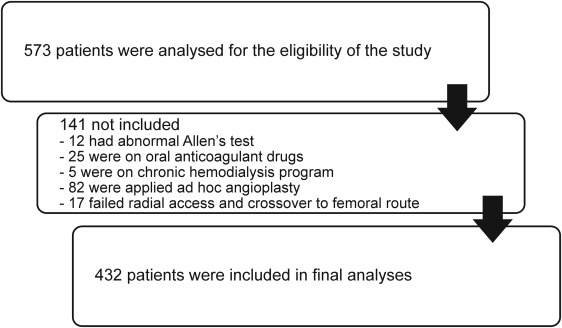
From January 2011 to January 2014, a total of 27,777 patients underwent coronary angiogram (57% transfemoral, 43% transradial) at our tertiary referral hospital. At initial analysis, 573 patients, aged from 18 to 80 years who were scheduled for elective coronary angiography and to whom an experienced cardiologist willed to proceed with radial access were included in this prospective and cross-sectional study. The operator was defined experienced if he or she had performed >1,000 transradial procedures in his or her career with >200 procedures per year. Exclusion criteria were as follows: having an abnormal Allen test result (n = 12), admission with acute coronary syndromes, oral anticoagulant drug usage (n = 25), being on chronic hemodialysis (n = 5), known to have severe hepatic disease, bleeding diathesis, coagulation disorders, previous history of CABG and ipsilateral use of both internal mammary and radial artery, and being performed ad hoc angioplasty (n = 82). Patients with failed radial access and crossover to femoral route were also excluded (n = 17; Figure 1 ).
After Allen test assessment, access site was sterilized, and local anesthesia with 2 to 3 ml of 2% prilocaine was administered. Radial artery cannulation was done with 6Fr hydrophilic 7-cm sheath (Primelife transradial set; Copper Medical Technology Co. Ltd., Shenzhen, China). After radial artery sheath insertion, to prevent vasospasm, 200 μg nitroglycerin and 5,000 IU UFH was injected into the radial artery. Six-French diagnostic coronary catheters (Boston Scientific) were used for coronary angiography.
On-site ACT measurements were performed at the end of the procedure just before the sheath removal with Hemochron device (International Technidyne Corp., Edison, New Jersey). When diagnostic angiography was completed, radial sheaths were removed, and a bandage made of a gauze pad was applied for local compression. One hour later, the bandage was slackened and kept on for 3 hours. After gaining patent hemostasis, all patients were discharged on the same day. The day after discharge, radial artery patency was evaluated by duplex ultrasonography (5 to 10 MHz; Siemens Elegra Ultrasonography Systems, Tokyo, Japan) by a single highly experienced examiner. Radial artery flow was assessed at the access site, at the wrist, and throughout forearm up to the brachial artery in the cross-sectional and the longitudinal axis. RAO was determined by detecting the absence of radial artery flow. On the basis of the findings of ultrasonography, the study population was divided into RAO and radial artery patent (RAP) groups. Hematomas were classified as grades 1 to 4 as described previously. Grade 3 and 4 hematomas were accepted as larger hematomas. The study was started after obtaining approval from the local ethics committee of our hospital. Informed consent was obtained from each patient.
SPSS 15.0 statistical software (SPSS Inc., Chicago, Illinois) was used for analysis. Descriptive statistics of the categorical variables were expressed as frequencies (n) and percentage (%). To test if continuous variables have normal distribution, Kolmogorov–Smirnov test was used. Continuous variables with normal distribution were expressed as mean ± SD. Continuous variables with normal distribution and categorical variables were compared by the Student t tests and chi-square independence test, respectively. Correlations were analyzed using the Pearson test. The optimal cut-off points of end-procedural ACT which discriminate groups (i.e., RAO vs RAP) from each other were evaluated by receiver operating characteristic (ROC) analysis, calculating area under the curve as giving the maximum sum of sensitivity and specificity for the significant test. For finding the independent predictors of RAO, we used multivariate logistic regression analysis. End-procedural ACT, radial artery diameter, and procedure duration were entered into the multivariate regression analysis. The p values <0.05 were considered significant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


