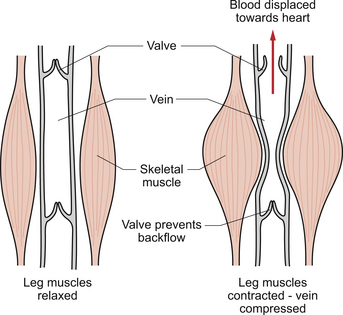
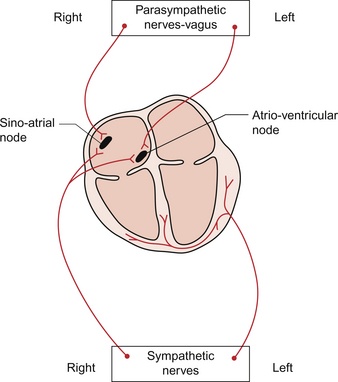
4 When the textbook person (see Chapter 1) is at rest their cardiac output, the volume of blood pumped by each side of the heart, is about 5 L per minute. In understanding how this is achieved the ‘rule of 70’ might be helpful. The heart typically beats at about 70 bpm and, when the ventricle empties it goes from a volume of about 140 mL at the end of the filling phase, diastole, to about 70 mL at the end of the contraction phase, systole. The ‘stroke volume’ is therefore about 70 mL and about 70 mL of blood remains in the ventricle at the end of each cardiac contraction. The ejection fraction of the heart, the stroke volume expressed as a percentage of end-diastolic volume, is thus typically about 50%. When appropriate an increase in the heart’s output can be achieved by a combination of an increase in heart rate and stroke volume. The maximum effective heart rate in the adult is about 180 bpm and the stroke volume can be increased both by filling the ventricle more during diastole and emptying it further during systole. In a very fit textbook person the maximum cardiac output is of the order of 25 L/min. When a person is upright, their head and shoulders are above the level of the heart but most of the rest of the body is below that level and thus gravity is largely a negative factor in determining venous return of blood to the heart. In a horizontal posture however the venous return will not be significantly opposed by gravity. For this reason if a person faints, it is usually best to leave them horizontal to aid the flow of blood back to the heart. Conversely, if a person has poor cardiac function a sitting position will decrease the venous return and hence the work load of the heart. Many people with cardiac problems sleep either in a chair or propped up in bed. The effect of gravity on venous pressure is further discussed in Chapter 10. The veins, especially in the limbs, are often to be found between major blocks of muscle. If muscle activity is increased, then the alternate compression and release of the veins will result in blood being propelled back towards the heart (Fig. 4.1). This mechanism is dependent on the presence of valves in veins in the lower limbs. This aspect of venous return is useful for guardsmen on parade. If they are standing still and upright over long periods of time there is a danger they will faint because their cardiac output, limited by the poor venous return, is not enough to supply their tissue’s needs especially on hot summer days when skin blood flow may be increased. They are told to move their toes in their boots and thus use the alternate contraction and relaxation of their leg muscles to aid venous return. The respiratory system has ‘dead space’ areas such as the nasal passages, trachea and bronchi which are ventilated but where no gas exchange takes place. This means that during exercise there is a functional advantage in keeping the respiratory rate relatively low and breathing deeply. The heart however is a through flow system and, within limits, an increase in heart rate will produce a proportionate rise in cardiac output, as long as the venous return is increased to provide the necessary blood to pump. This is true in an adult up to a heart rate of about 180 bpm. If the heart rate goes much above this value then cardiac output falls precipitously because there is an encroachment on the ‘rapid filling time’—that period of time which immediately follows the end of ventricular systole and when most of the ventricular filling occurs (see Chapter 3). The result is that excessively high heart rates are associated with a reduced stroke volume. Small minute to minute changes in cardiac output, as might be associated with mild exercise such as walking, tend to be achieved largely by changes in both heart rate and stroke volume (see Chapter 13). Changes in stroke volume reach maximum levels at fairly moderate exercise intensity and the further increases during heavy exercise are achieved just with heart rate changes. The effects of exercise on cardiac function are considered in more detail in Chapter 13. There is considerable variation in the resting heart rate in the adult population with a normal range of 50–100 bpm. As explained in Chapter 2 the rate of beating of the heart is normally determined by the pacemaker at the sinoatrial node (SAN). The rate of this pacemaker is modulated by both the sympathetic and parasympathetic nervous systems. At rest the parasympathetic inhibition dominates so that the typical resting heart rate of about 70 bpm is less than the natural intrinsic rate of the SAN which is about 110–120 bpm (see Chapter 2). Small increases in heart rate, such as might occur during walking, are produced by inhibition of the parasympathetic tone. If the heart rate is to go above about 110 bpm, then an increased sympathetic nerve activity is also required. The role of the central nervous system control centres and the function of the baroreceptor reflex in the control of heart rate are further discussed in Chapter 10. The sympathetic innervation of the heart is routed via the cervical and stellate sympathetic ganglia. It is the sympathetic fibres on the right side of the body which have the major effect on heart rate (Fig. 4.2). The fibres from the left side of the sympathetic nervous system are more concerned with the regulation of cardiac contractility. The noradrenaline (norepinephrine) released at the nerve endings acts on β1 receptors in the SAN and increases the Ca++ current in phase 4 of the SAN action potential. This accelerates the rate of firing of the SAN cells (see Chapter 2). The parasympathetic innervation of the pacemaker tissue is via the left and right branches of the vagus nerve but, like the sympathetic innervation, the fibres are distributed differentially (Fig. 4.2). The right vagus goes mainly to the SAN with a small innervation of the atrioventricular node (AVN) whereas the left vagus goes primarily to the AVN with only a small outflow to the SAN. The vagal fibres to the heart originate in the dorsal motor nucleus of the vagus or in the nucleus ambiguus (see Chapter 10). The parasympathetic ganglia, the location of the nerve cell bodies, are on the cardiac surface or within the heart itself and the short postganglionic fibres release acetylcholine as their neurotransmitter. This acetylcholine acts on muscarinic (M2) receptors in the SAN and, via an inhibitory G protein mechanism, reduces the production of cAMP within the cell. Cyclic AMP activates populations of Na+ channels and L-type Ca++ channels causing depolarization of the pacemaker cells. Inhibiting cAMP formation therefore reduces the rate of depolarization and slows the heart rate. There is also a hyperpolarizing effect produced following binding of acetylcholine to M2 receptors. This is mediated by activation of a population of K++ channels. As a result the membrane potential is moved closer to the potassium equilibrium potential (EK) of −94 mV and therefore further away from the threshold at which an action potential is triggered (see Chapter 2). The right and left vagus nerves have little effect on cardiac contractility. The heart is an unusual form of pump in that not only is it able to change the rate at which it pumps but, if necessary, it is also able to change the volume of blood pumped at each stroke. Under resting conditions, the ventricles in the adult heart typically fill to about 140 mL (the end-diastolic volume) and empty to about 70 mL (the end-systolic volume) giving rise to a stroke volume of about 70 mL.However as the normal range of heart rate is quite wide at 50–100 bpm, individuals with a slow resting heart rate will operate with a stroke volume greater than 70 mL and people with a fast heart rate will have a correspondingly smaller resting stroke volume. Resting cardiac output will therefore be comparable between individuals with the same body size irrespective of resting heart rate. An outline of the case history of a man with increased stroke volume in his heart is described in Case 4.1:1.
REGULATION OF CARDIAC FUNCTION
Introduction

Venous return
The skeletal muscle pump
Control of cardiac output

Regulation of heart rate
Regulation of stroke volume
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine