Thoracic aortic dilatation requires accurate and timely detection to prevent progression to thoracic aortic aneurysm and aortic dissection. The detection of thoracic aortic dilatation necessitates the availability of cut-off values for normal aortic diameters. Tools to evaluate aortic dimension above the root are scarce and inconsistent regarding age groups. The aim of this study was to provide reference values for aortic root and ascending aortic diameters on the basis of transthoracic echocardiographic measurements in a large cohort of children and adults. Diameters at the level of the sinuses of Valsalva (SoV) and ascending aorta (AA) were assessed with transthoracic echocardiography in 849 subjects (453 females, age range 1 to 85 years, mean 40.1 ± 21.3 years) and measured according to published guidelines. Linear regression analysis was applied to create nomograms, as well as equations for upper limits of normal and z-scores. SoV and AA diameters were strongly correlated with age, body surface area (BSA), and weight (r = 0.67 to 0.79, p <0.001 for all). Male subjects had significantly larger aortic dimensions at all levels in adulthood, even after BSA correction (p ≤0.004 for all age intervals). Gender-, age-, and BSA-specific upper limits of normal and z-score equations were developed from a multivariate regression model, which strongly predicts SoV and AA diameters (adjusted R 2 for SoV = 0.84 and 0.67 and for AA = 0.82 and 0.74, for male and female subjects, respectively). In conclusion, this study provides widely applicable reference values for thoracic aortic dilatation screening purposes. Age, BSA, and gender must be taken into account when assessing an individual patient.
Correctly defining aortic dilatation requires upper limits of normal (ULNs) for aortic diameters. Aortic dilatation is defined as a diameter of 1.96 standard errors of the estimate (SEEs) above the predicted diameter for a specific patient. Dilatation of the proximal thoracic aorta, defined as the segment of the aorta between the aortic valve and the brachiocephalic artery, is frequently encountered in distinct pathologies such as heritable aortopathies (e.g., Marfan syndrome and Loeys-Dietz syndrome), Turner syndrome, and bicuspid aortic valve syndrome, but it also occurs in the setting of degenerative aortic disease. As dilatation progresses, it confers risk for aortic valve regurgitation and/or aortic dissection, the latter of which is associated with considerable morbidity and mortality. Because initially published nomograms used to predict normal proximal thoracic aortic diameters for body surface area (BSA), age, and/or gender were based on small reference populations with varying age groups, Devereux et al recently published reference values for sinuses of Valsalva (SoV) diameters obtained in a large cohort of normal subjects aged 15 to 86 years. Until now, however, very limited 2-dimensional echocardiographic data on the ascending aorta (AA) over a wide age range are available. With this study, we aimed to provide uniform guidelines for evaluation of the aortic diameters at the SoV and AA on the basis of echocardiographic measurements in a large cohort of children and adults ranging from 1 to 85 years of age.
Methods
Patients who underwent routine cardiovascular checkups in the context of family screening for genetic disease, preoperative evaluation for noncardiovascular surgery, cardiovascular evaluation to obtain permission for sports activities, or exclusion of pericarditis or endocarditis, as well as patients under follow-up at the outpatient clinic of the cardiology department for various reasons, other than aortopathy, requiring cardiac ultrasound (previous chemotherapy, rheumatic disorders, arrhythmia, or coronary artery disease), were included in this analysis. Patients with bicuspid aortic valves, significant valvular disease, or evidence of connective tissue disorders, such as Marfan syndrome, were excluded. All subjects underwent echocardiographic examinations at the pediatric or adult cardiology department of Ghent University Hospital from February 2008 to June 2013. Height and weight were measured, and BSA was calculated according to the formulas of Du Bois and Du Bois (BSA DB ) and Haycock et al (BSA H ). Blood pressure (BP) was measured before the ultrasound examination using a validated oscillometric BP device (HEM-907; Omron Healthcare, Kyoto, Japan). Transthoracic echocardiography was performed by experienced adult and pediatric cardiologists using commercially available ultrasound equipment (Vivid 7; GE Vingmed Ultrasound AS, Horten, Norway) with adequate multifrequency transducers, ranging from 3.5 to 8 MHz for children and from 2 to 5 MHz for adults. Standard 2-dimensional parasternal long-axis, short-axis, and apical views of the proximal thoracic aorta, left ventricle, and left atrium were recorded. Color Doppler and continuous Doppler were used for the evaluation of valvular function. All proximal aortic diameters were assessed on 2-dimensional images in the parasternal long-axis view at end-diastole from leading edge to leading edge. The diameter of the AA was assessed at the level of the right pulmonary artery ( Supplementary Figure 1 ). All aortic measurements were performed off-line by 3 experienced readers (JDB, LD, and LC). Interobserver variability is presented in Supplementary Table 1 . This study was approved by the local ethics committee.
Gender differences for body size parameters (height, weight, BSA DB , BSA H , and body mass index [BMI]), systolic BP, diastolic BP, and proximal aortic dimensions were analyzed with the unpaired-sample Student’s t test for normally distributed continuous variables and with the Mann-Whitney U test for variables not normally distributed. Gender differences for aortic dimensions, adjusted for BSA DB , were further analyzed in subgroups, with an age interval of 5 years before the age of 15 years and an age interval of 10 years after the age of 15 years, to investigate gender-related differences before and during puberty compared with after puberty.
Correlation coefficients and univariate relations of morphologic parameters (weight, height, BSA, and BMI), age, BP, and SoV and AA diameters were assessed. For homogeneity of variance, the values of the aortic diameters, age, and morphologic parameters were transformed if necessary. Linear regression statistics were then applied. A spline regression model was computed with a spline knot set at the age of 15 years to allow a change in the regression slope due to the transition of a child to an adult. To correct for obesity (defined as BMI >95th percentile for subjects ≤18 years of age [using charts provided by the Centers for Disease Control and Prevention] and BMI >30 kg/m 2 for subjects >18 years of age) within the cohort, obesity as a categorical variable was added to the model, together with an interaction term for obesity and BSA. Model selection was based on adjusted R 2 values. Residual and regression diagnostic analyses were performed. The relation between standardized residuals of the linear regression models, body size parameters, and age was determined. After model selection, formulas and nomograms for ULNs and z-score calculations for the 2 aortic diameters were computed for male and female subjects. The ULN was defined as >1.96 SEEs greater than the mean predicted natural logarithm of the aortic diameter measured at the level of the SoV or AA (log10[Ao]) (ULN = 10 [mean predicted log10(Ao) + 1.96SEE] ), and the z-score was defined as the number of SEEs greater than or less than the mean predicted log10(Ao) (z = [measured lg10(Ao) − mean predicted log10(Ao)]/SEE). The cutoff for aortic dilatation was set at a z-score >1.96 SEEs or the ULN >1.96 SEEs of the mean predicted log10(Ao). Results are presented as mean ± SD. Two-tailed p-values <0.05 were considered statistically significant.
Results
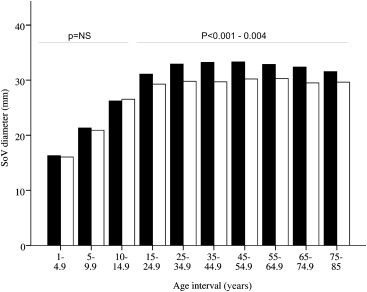
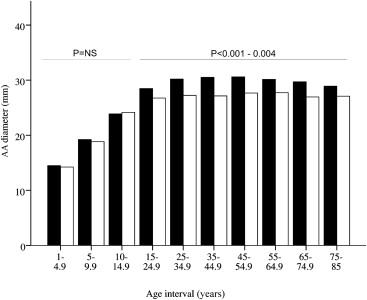
We included 849 Caucasian subjects (453 females, age range 1 to 85 years, mean 40.1 ± 21.3, median 40.8 years). In all but 5 adult subjects, the AA diameter could be assessed. As shown in Supplementary Figures 2 and 3 , all age decades and BSA categories are well represented. Body size parameters, BPs, age, and proximal thoracic aortic dimensions are listed in Table 1 . The study population consisted of 12.8% patients with hypertension (109 of 849) (22.4% [108 of 483] in the subgroup aged ≥35 years). Most patients (95.4%) were adequately treated with antihypertensive medications. Plotting aortic diameters (SoV and AA) and body size parameters (height, weight, BSA DB , and BSA H ) against age indicated a faster increase in aortic dimensions before the age of 15 years, which was correlated with the increases in body size parameters before the age of 15 years ( Figure 1 ). The change in diameter was similar for the SoV and AA as a function of age. From the age of 15 years on, BSA DB -adjusted SoV diameters increased on average by 1.1 ± 0.5 and 0.9 ± 0.4 mm per decade for male and female subjects, respectively, and on average by 1.3 ± 0.6 and 1.2 ± 0.5 mm for BSA DB -adjusted AA diameters (assessed with our multivariate models; see the following discussion). Proximal thoracic aortic diameters at all levels were significantly higher in male subjects in the entire group (p ≤0.001 for all diameters; Table 1 ). When the subgroup of pre- and peripuberty children (aged <15 years) was considered, we found only a small, borderline-significant gender difference at the level of the AA (18.9 ± 2.9 and 17.8 ± 3.2 mm for male and female subjects, respectively, p = 0.048). Analysis of covariance, with BSA DB adjustment, indicated that the gender differences remained statistically significant for those ≥15 years of age for the SoV and the AA (p <0.001 to 0.004; Figures 2 and 3 ). In contrast, below the age of 15 years, there were no significant gender differences after BSA DB adjustment ( Figures 2 and 3 ). Male subjects had on average, over all age decades ≥15 years, 2.4 ± 0.3 and 1.4 ± 0.3 mm larger BSA DB – and age-adjusted SoV and AA diameters, respectively (assessed with our multivariate models; see the following discussion).
| Variable | Total | Males | Females | ||
|---|---|---|---|---|---|
| (N = 849) | <15y (N = 80) | ≥15y (N = 316) | <15y (N = 53) | ≥15y (N = 400) | |
| Age (years) | 40.1 ± 21.3 | 8.5 ± 3.6 | 45.2 ± 18.1 | 8.1 ± 3.6 | 46.6 ± 17.4 |
| Systolic BP (mmHg) | 129.5 ± 17.3 | 110.3 ± 13.3 | 134.3 ± 14.8 † | 108.3 ± 13.6 | 129.1 ± 17.2 † |
| Diastolic BP (mmHg) | 72.3 ± 11.2 | 63.3 ± 10.5 | 73.7 ± 11.7 | 63.4 ± 9.0 | 72.6 ± 10.4 |
| Height (cm) | 164.5 ± 19.5 | 132.9 ± 25.7 | 177.4 ± 8.3 † | 130.7 ± 25.4 | 165.0 ± 7.2 † |
| Weight (kg) | 64.5 ± 19.5 | 31.1 ± 14.3 | 77.7 ± 13.6 † | 30.3 ± 14.0 | 65.3 ± 11.7 † |
| Body surface area DB (m 2 ) | 1.7 ± 0.4 | 1.1 ± 0.3 | 1.9 ± 0.2 † | 1.0 ± 0.3 | 1.7 ± 0.2 † |
| Body surface area H (m 2 ) | 1.7 ± 0.4 | 1.1 ± 0.3 | 2.0 ± 0.2 † | 1.0 ± 0.3 | 1.7 ± 0.2 † |
| Body mass index (kg/m 2 ) | 23.1 ± 4.8 | 16.6 ± 2.7 | 24.7 ± 4.1 ∗ | 16.7 ± 2.6 | 24.0 ± 4.2 ∗ |
| Annulus (mm) | 19.6 ± 3.0 | 15.6 ± 2.9 | 21.8 ± 2.1 † | 14.8 ± 2.5 | 19.2 ± 1.9 † |
| Sinuses of Valsalva (mm) | 29.7 ± 5.4 | 21.6 ± 3.7 | 33.4 ± 3.8 † | 20.6 ± 3.7 | 29.4 ± 3.4 † |
| Sinotubular junction (mm) | 25.4 ± 5.1 | 17.3 ± 3.0 | 28.5 ± 3.7 † | 16.8 ± 3.2 | 25.5 ± 3.2 † |
| Ascending aorta (mm) | 27.1 ± 5.5 | 18.9 ± 2.9 ∗ | 30.0 ± 4.3 † | 17.8 ± 3.2 ∗ | 27.7 ± 3.9 † |
† p-value <0.001 for the difference between males and females.

Aortic dimensions at the level of the SoV and AA were most strongly correlated with age, BSA (both BSA DB and BSA H ), and weight (r = 0.67 to 0.79, p <0.001 for all comparisons; Supplementary Table 2 ). Height yielded a strong correlation with aortic dimensions in children; in male and female subjects ≥15 years of age, height was only weakly correlated with aortic dimensions. Formulas for z-score and ULN calculation of the SoV and AA diameters were assessed using multiple regression for male and female subjects separately. The multivariate model with BSA and age (SoV, AA, and age were transformed to their natural logarithms) was selected on the basis of excellent adjusted R 2 values (0.84 and 0.67 for the SoV and 0.82 and 0.74 for the AA, for male and female subjects, respectively; Supplementary Table 3 ). A model for BSA DB and BSA H was computed. There were no significant linear relations between standardized residuals and BSA DB , BSA H , weight, and age (r = −0.047 to 0.051, p >0.28 for all comparisons). The distribution of the standardized residuals was not different between children and adults.
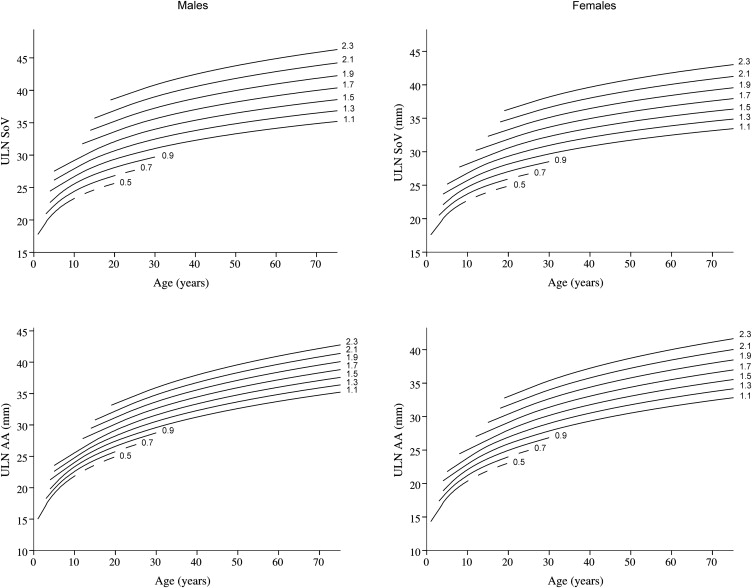
Nomograms displaying the ULN for SoV and AA diameters as a function of BSA DB are presented in Figure 4 , and ULN values are presented in Supplementary Table 4 . Equations providing the ULN and z-score as a function of BSA and age are listed in Table 2 . There were no significant differences in the ULN for SoV and AA using BSA DB compared with the ULN using BSA H for the total population (p = 0.77 to 0.93) or for the subgroup of patients with BSA H ≤0.7 m 2 (p = 0.60 to 0.84). We applied different previously published formulas to the data set of patients included in this study to determine agreement with ULN values computed with the formulas we propose here. The differences between ULN values calculated with the various formulas are presented in Supplemental Table 5 . Our values correlate well and lie within the range of those calculated with the other available formulas. In particular, the small differences between the ULNs of SoV and AA dimensions calculated with our formula and those of Devereux and Gautier et al, respectively, are notable.
| Aortic Level | Gender | Upper Limit of Normal Equation | Z-score Equation |
|---|---|---|---|
| SoV | Male | 10 ˆ ( 1.108 + 0.136 x L g 10 ( A g e ) + 0.099 x B S A D B + 1.96 x 0.0381 ) | ( L g 10 ( S o V ) − ( 1.108 + 0.136 x L g 10 ( A g e ) + 0.099 x B S A D B ) ) / 0.0381 |
| 10 ˆ ( 1.115 + 0.137 x L g 10 ( A g e ) + 0.094 x B S A H + 1.96 x 0.0388 ) | ( L g 10 ( S o V ) − ( 1.115 + 0.137 x L g 10 ( A g e ) + 0.094 x B S A H ) ) / 0.0388 | ||
| Female | 10 ˆ ( 1.100 + 0.129 x L g 10 ( A g e ) + 0.091 x B S A D B + 1.96 x 0.0421 ) | ( L g 10 ( S o V ) − ( 1.100 + 0.129 x L g 10 ( A g e ) + 0.091 x B S A D B ) ) / 0.0421 | |
| 10 ˆ ( 1.112 + 0.132 x L g 10 ( A g e ) + 0.080 x B S A H + 1.96 x 0.0427 ) | ( L g 10 ( S o V ) − ( 1.112 + 0.132 x L g 10 ( A g e ) + 0.080 x B S A H ) ) / 0.0427 | ||
| AA | Male | 10 ˆ ( 1.033 + 0.188 x L g 10 ( A g e ) + 0.070 x B S A D B + 1.96 x 0.0431 ) | ( L g 10 ( A A ) − ( 1.033 + 0.188 x L g 10 ( A g e ) + 0.070 x B S A D B ) ) / 0.0431 |
| 10 ˆ ( 1.038 + 0.187 x L g 10 ( A g e ) + 0.068 x B S A H + 1.96 x 0.0433 ) | ( L g 10 ( A A ) − ( 1.038 + 0.187 x L g 10 ( A g e ) + 0.068 x B S A H ) ) / 0.0433 | ||
| Female | 10 ˆ ( 1.001 + 0.177 x L g 10 ( A g e ) + 0.086 x B S A D B + 1.96 x 0.0453 ) | ( L g 10 ( A A ) − ( 1.001 + 0.177 x L g 10 ( A g e ) + 0.086 x B S A D B ) ) / 0.0453 | |
| 10 ˆ ( 1.006 + 0.172 x L g 10 ( A g e ) + 0.087 x B S A H + 1.96 x 0.0450 ) | ( L g 10 ( A A ) − ( 1.006 + 0.172 x L g 10 ( A g e ) + 0.087 x B S A H ) ) / 0.0450 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


