Familial aortic aneurysm (AA) is mostly inherited as an autosomal dominant disorder. However, recessively inherited AA has also been observed but in association with skin manifestations of cutis laxa, which is caused by a mutated EFEMP2 gene. In the present study, we recruited 9 patients, from 4 unrelated consanguineous families, with recessively inherited AA. The index cases, their parents, and siblings underwent clinical evaluation and cardiac imaging. In the affected subjects, the clinical presentation ranged from sweating and cyanosis at 3 months of age to incidental findings in an asymptomatic adult. The echocardiogram revealed a wide spectrum of severity of the AA, with a Z-score varying from 5 to 33. Intrafamilial variability was also evident; 2 unrelated subjects were detected at 17 and 20 years of age through family screening. The skin manifestations of cutis laxa were not found in any patient. In 1 family, genome-wide single-nucleotide polymorphism analysis detected a homozygous block, shared by 2 affected siblings, on chromosome 11 at q13. Sequence analysis of EFEMP2 , located on chromosome 11 at q13, identified a novel homozygous mutation (p.E161K) in all 9 affected subjects. In this largest cohort of reported patients with a mutated EFEMP2 gene, we illustrate the phenotypic spectrum of inherited AA due to a novel EFEMP2 mutation. In conclusion, our work suggests that in families with apparently recessively inherited AA, molecular analysis of EFEMP2 gene might be warranted.
In the present study, we performed single-nucleotide polymorphism (SNP)-based genome-wide analysis on a consanguineous family with 2 children with severe aortic root and ascending aorta aneurysm in the absence of the skin manifestations of cutis laxa. A homozygous block on chromosome 11 at q13, where the EFEMP2 gene is located, was found to be shared by the affected children. Sequencing EFEMP2 identified a novel homozygous mutation, which was also detected in 7 patients from 3 other families. To date, only 6 patients with mutations in the EFEMP2 gene have been reported. It has been suggested that a mutated EFEMP2 gene impairs the stability and/or secretion of fibulin-4, leading to defective elastogenesis because of the decrease in protein in the extracellular matrix. To our knowledge, our work represents the largest cohort of patients with the EFEMP2 mutation.
Methods
Nine patients, from 4 unrelated consanguineous families, were recruited through the Cardiovascular Genetics Program at King Faisal Specialist Hospital and Research Centre (Riyadh, Saudi Arabia). The index case in each family was referred to us for evaluation of aortic aneurysm (AA). The index cases and their parents and siblings underwent clinical evaluation and transthoracic echocardiography. A parasternal long-axis measurement of the aortic root and ascending aorta with a Z score >2 was considered abnormal. Patients found to have dilated aortic root and/or ascending aorta also underwent cardiac magnetic resonance imaging. The Research Advisory Counsel at KFSH&RC approved the present study.
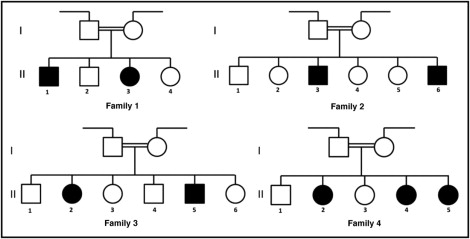
After obtaining informed consent, blood samples were collected from all affected patients, their parents, and their unaffected siblings. Genomic DNA was extracted for each sample by standard salt-precipitation methods. In 1 consanguineous family (family 1, Figure 1 ) , SNP-based genotyping was performed for the 2 affected children, their parents, and their 2 unaffected siblings using Axiom CEU Human Array from Affymetrix (Santa Clara, California). To detect the regions of homozygosity, SNPs were analyzed using AutoSNPa software.
In all 4 families, the genomic DNA of the affected patients, their parents, and their siblings was amplified using polymerase chain reaction using intronic primers designed to flank (50 to 100 bp) the coding exons, as defined by the Ensembl Genome Browser of EFEMP2 ( NG_012304 ). Purified polymerase chain reaction amplicons were directly sequenced with the dideoxy chain-termination method using an ABI Prism Big Dye Terminator, version 3.1, Cycle Sequencing Kit according to the manufacturer’s instructions and processed on an ABI 3730XL capillary sequencer (Applied Biosystems, Foster City, California). Sequence analysis was performed using the SeqMan 6.1 module of the Lasergene (DNA Star, Madison, Wisconsin) software package and then compared to the reference GenBank sequence.
Results
Nine patients (age 3 months to 20 years), from 4 unrelated families who reside in the same region in Saudi Arabia, were found to be affected ( Figure 1 and Table 1 ). The clinical presentation ranged from sweating and cyanosis at 3 months of age to an incidental finding in an asymptomatic adult. All patients exhibited severe AA with a Z score from 5 to 33. All affected subjects had cardiac magnetic resonance imaging findings consistent with the echocardiographic findings ( Figures 2 and 3 ) . The typical skin features of cutis laxa were not found in any of the affected patients. With the exception of a 20-year-old patient, all affected subjects underwent surgical intervention with resection of the ascending aorta and replacement. Aortic tissue from all 8 patients was submitted for histopathologic examination, which revealed medial degeneration with elastic tissue fragmentation and loss ( Figure 4 ) . Areas with loss of elastic tissue were filled with amorphous extracellular matrix, imparting a cystic appearance within the media of the vessel wall.
| Family | Patient | Age at Presentation (y) | Clinical Presentation | Ascending Aorta Diameter (cm) | Z Score | Age at Surgical Intervention (y) |
|---|---|---|---|---|---|---|
| 1 | II-1 | 3 | Heart murmur | 3.6 | 8.9 | 3 |
| II-3 | 1.3 | Wheezing | 3.7 | 13.0 | 3.5 | |
| 2 | II-3 | 17 | Asymptomatic | 6.6 | 15.8 | 17 |
| II-6 | 8 | Asymptomatic | 8.2 | 33.0 | 8 | |
| 3 | II-2 | 20 | Asymptomatic | 3.5 | 5.0 | — |
| II-5 | 5 | Heart murmur | 4.0 | 11.3 | 5 | |
| 4 | II-2 | 0.25 | Sweating, cyanosis | 3.6 | 11.4 | 0.67 |
| II-4 | 0.3 | Dyspnea | 6.6 | 15.8 | 1.5 | |
| II-5 | 2.5 | Asymptomatic | 4.3 | 16.0 | 2.5 |



