Radiofrequency Ablation of Barrett’s Esophagus
Shajan Peter
C. Mel Wilcox
Klaus Mönkemüller
DEFINITION
Barrett’s esophagus (BE) is an acquired condition due to a change in the normal esophageal squamous epithelium to columnar epithelium containing goblet cells. This metaplastic change can progress to low-grade dysplasia (LGD) and high-grade dysplasia (HGD), with the latter having a 5% to 10% risk of developing into esophageal adenocarcinoma.1,2
Radiofrequency ablation (RFA) is a safe and effective endoscopic treatment modality for BE whereby squamous tissue replaces the ablated metaplastic or dysplastic epithelium. RFA uses a bipolar electrode array to generate thermal energy to result in tissue dissipation.3
PATIENT HISTORY AND PHYSICAL FINDINGS
It might be difficult to distinguish symptoms of BE from gastroesophageal reflux disease (GERD) clinically, although increased duration, severity, and early age of onset for reflux symptoms as well as obesity predispose to BE occurrence.4
Age older than 55 years, male gender, white ethnicity, or smokers are predisposing factors for BE development and progression to dysplasia. Genetic influences may play a role, although only a small proportion (7%) of patients with BE have a documented family history of BE or esophageal cancer.5
Selection of patients for endoscopic treatment of BE requires a multidisciplinary approach consisting of the endoscopist, pathologist, and the surgeon.
Confirmation of dysplasia (high or low grade) on biopsies or endoscopic mucosal resection (EMR) specimens is done by a dedicated gastrointestinal (GI) pathologist.6
IMAGING AND OTHER DIAGNOSTIC STUDIES
Detailed endoscopic examination with high-definition white light of the BE segment is essential for management.
The extent of the BE segment should be defined using the Prague C & M classification including the length of the circumferential segment (C) and the maximal extent of the BE segment (M)7 (FIG 1).
Other imaging modalities that might help in delineating BE are narrow band imaging (NBI), chromoendoscopy, autofluorescence imaging, and confocal laser endoscopy. These adjuncts aid in directed biopsies.
Any visible lesions in the Barrett’s segment should be described using the Paris classification.8
Targeted biopsies are obtained from visible abnormalities, followed by four-quadrant biopsies of every 1 to 2 cm of the BE segment (Seattle protocol) and these should be reviewed by a dedicated GI pathologist.9 Nodular lesions are best staged by an EMR as described in Chapter 28.
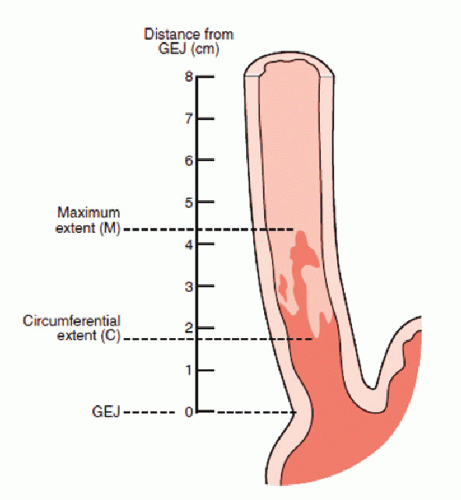 FIG 1 • Prague C & M classification. |
ENDOSCOPIC MANAGEMENT
Preoperative Planning
Patients are given standard esophagogastroduodenoscopy (EGD) preprocedure preparation instructions with specific attention to factors that increase risk of sedation including morbidly obese patients; anatomic variants such as short neck, cervical osteophytes, cricopharyngeal hypertrophy; and prior history of surgery involving the GI tract, radiation, or documentation of previous strictures.
No antibiotics are required and it is desirable to minimize or stop antiplatelet/anticoagulation prior to the procedure.
Positioning
The patient is placed in the left lateral decubitus position and prepared as for a routine upper endoscopy.
Table 1: Circumferential Ablation Equipment List | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
Table 2: Focal Ablation Equipment List | |||||||
|---|---|---|---|---|---|---|---|
|
CIRCUMFERENTIAL ABLATION
Endoscopy with Inspection and Recording the Landmarks
Measurements are taken to map the extent of the BE showing (1) top of intestinal metaplasia (TIM), (2) proximal contiguous area of BE (M), (3) proximal level at which the BE is circumferential, (4) and the top of the gastric folds (TGF) (FIG 2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


