Quantification of Left Ventricular Systolic and Diastolic Function
Christopher L. Holley
High-Yield Findings
Normal LV size: PLAX diameter <5.3 cm♀, 5.9 cm ♂; apical four-chamber end diastolic volume indexed to BSA ≤75 mL/m2
Normal LV systolic function: Ejection fraction ≥55%
Normal LV mass indexed to BSA: <89 mL/m2♀, <103 mL/m2♂
Normal LA size indexed to BSA: <22 +/- 6 mL/m2
Normal diastolic function is quickly assessed by TDI of the mitral annulus; e′ lateral ≥10 cm/s or medial ≥8 cm/s
Key Views
Parasternal long axis: 2D (linear) measurements of LV, LA, and aortic root
Parasternal short axis: Assessment of LV mass
Apical four chamber: Tracings for LV and LA volumes; Doppler assessment of mitral inflow and annular velocities
Introduction
Accurate quantitative assessment of the left ventricle (LV) is an essential aspect of echocardiography. At the time of interpretation, indexed measurements (to BSA or height) should be used in reports, as “normal” measurements vary significantly by gender and body size.
Tips for Optimizing Image Quality:
Tips for Interpreting Studies:
Qualitative size and function estimates should be avoided except as a “reality check” for measured values.
Use multiple views for assessment.
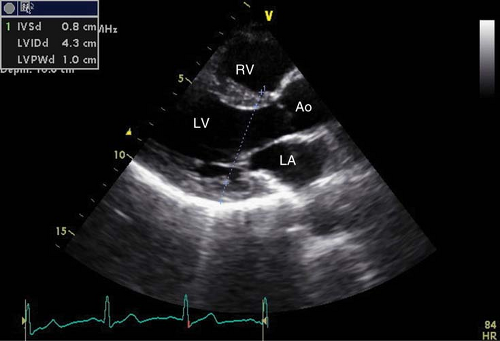
Figure 4-1. Parasternal long-axis view with linear left ventricular measurements performed at the level of the mitral valve leaflet tips.
Beware of off-axis views as they may distort the comparative size of chambers and not allow use of standardized normal ranges.
LV Dimensions
Parasternal long axis (PLAX)
At a minimum, make simple linear measurements and compare to (non-indexed) upper limits of normal (Fig. 4-1 and Table 4-1)
LVID (“minor axis,” LVIDd and LVIDs, measured at MV leaflet tips in end-diastole and end-systole respectively)
Septal and inferolateral wall thicknesses (measured at MV leaflet tips in end-diastole)
Table 4-1 Linear Dimensions
LVIDd (cm)
SWT or PWT (cm)
RWT
Aorta (cm)
LA (cm)
Upper normal
5.3 ♀, 5.9 ♂
1
0.42
4a
4
Severely abnormal
≥6.3
≥1.7
≥0.53
§
≥5.2
aIndicates wide variance with age and BSA. (Adapted from Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463).
§ See Figure 4-2.
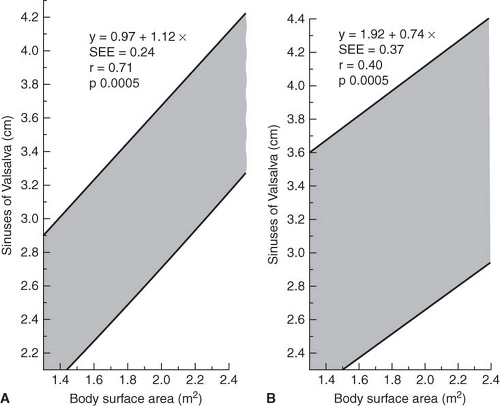
Figure 4-2. Ninety-five percent normal confidence intervals for aortic root dimension at the sinuses of Valsalva indexed to body surface area for adults <40 years of age (A) and those ≥40 years (B). (Reprinted from Roman MJ, Devereux RB, Kramer-Fox R, et al. Two-dimensional echocardiographic aortic root dimensions in normal children and adults. Am J Cardiol. 1989;64:507–512, with permission from Elsevier.)
Aortic (Ao) root diameter, at the sinuses, sinotubular junction and proximal ascending aorta (see Chapters 9 and 10) (Fig. 4-2)
LA size is more accurately measured as a volume in the A4C rather than linear dimensions in the PLAX view
M-mode measurements may be used although beware of errors related to beam angle (Fig. 4-3)
Apical views (A4C and A2C)
The minimum assessment should include LA volume assessment and measurement of LV volume in systole and diastole for LV ejection fraction (Table 4-2)
The LA is measured at end-systole tracing from the MV annulus and excluding the pulmonary veins and LA appendage.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


