Fig. 21.1
After deliberate overstenting of the left pulmonary artery, an ultrahigh-pressure balloon was inserted across the struts and dilated to its nominal diameter, breaking the stent struts at about 8 atm dilation pressure to achieve unrestricted access to the left pulmonary artery
A special issue is the treatment of bilateral bifurcation stenosis. To overcome the problem of obstructing the contralateral vessel by stent implantation, a simultaneous implantation of two stents in each side can be performed.
The disadvantage is, however, that the creation of a double lumen in the pulmonary trunk might be an obstacle for interventional treatments like pulmonary valve implantation.
An alternative concept is the creation of a Y-stent, in which two stents were placed through their meshes directly into the bifurcation (Fig. 21.2).
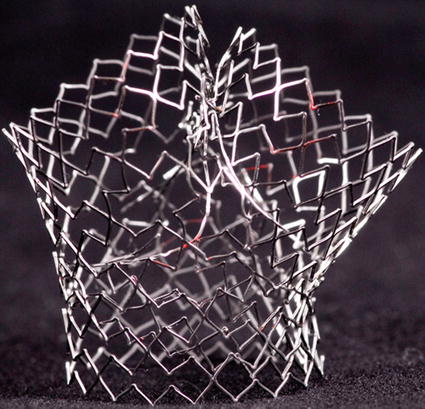
Fig. 21.2
A Y-stent, created from two balloon-expandable stents, which were placed across the struts of each other and consecutively dilated with an ultrahigh-pressure balloon (see Fig. 21.1) to achieve unrestricted flow and access into both branches
For this indication, preferably large open-cell design stents are used. Free access without jailing of a vessel is possible because stent struts can be cracked open by ultrahigh-pressure balloons at about 9–14 atm – a fact which has considerably lowered the threshold to overstent a pulmonary branch.
21.7 Materials
After angiographic depiction and exact measurements of the target lesion, a distal guide wire position has to be achieved.
This is done with an end open catheter (e.g., Arrow wedge catheter 4–7 F, Judkins right coronary catheter, multipurpose catheter).
Balloon catheters are less prone to get caught in tricuspid valve chordae on their way up to the pulmonary arteries.
Terumo guide wires (0.018, 0.025, 0.035) straight or curved can be very helpful to reach this distal position.
In infants and small children, a coronary guide wire (e.g., BMW universal guide wire (Abbot) 0.014) may be helpful.
This wire is then exchanged for a stiffer guide wire (Amplatz extra or ultra-stiff wire (Cook medical) 0.035/0.025); in adults and adolescents even a stronger wire may be needed (Meier wire Boston Scientific 0.035, Lunderquist Cook medical 0.035). The Meier wire has a rather long soft tip which is shorter in the Lunderquist wire.
The Multitrack catheter (PFM) may be used for pullback assessment and for angiograms without losing guide wire position.
If only a balloon angioplasty is planned, a short sheath of adequate size is sufficient.
For stent placement and cutting balloons, a long sheath needs to be placed across the target lesion.
Stents augment the external balloon diameter by 1 or 2 French sizes depending on the stent type.
Typically used sheaths are Flexor (Cook) 5 F–10 F (70–80 cm), Arrow-Flex (Arrow) 6 F–11 F (45–80 cm), and Mullins Sheath straight and curved (Cook) (5–22 F)(63–85 cm); coronary guiding catheters (5–8 F) may also be useful.
Common balloons for angioplasty and stent deployment are Powerflex (Cordis) (6–12 mm; 2–4 cm), VACS (Osypka) (9–30 mm, 2–6 cm), and Z-med/BiB (NuMed)(10–30; 2.5–6 cm).
For resistant lesions, ultrahigh-pressure Kevlar balloon are used: Dorado (Bard) (8–10 mm 2 cm)/Atlas Gold (Bard)(12–24 mm, 2–4 cm) or the Mullins (NuMed) (12–25 mm; 4 cm) balloons are available.
Various stents (usually balloon expandable, premounted, or hand crimped) are used.
For stenting of segmental pulmonary arterial stenosis, premounted coronary bare metal stents can be implanted. These small stents can only be enlarged by 1 or 2 mm and hence cannot reach large diameters.
Premounted stents at medium size are, for example, the Cordis Palmaz stents on Opta balloon (on 5–10 nm balloons). These stents can be dilated up to 12 mm.
The Cook formula stent is a rather new premounted stent crimped on a 6, 8, and 10 mm balloon. The largest stents can be dilated up to 16 mm. It offers, however, the possibility to reach unlimited diameters by overdilation with ultrahigh-pressure balloons. The stent struts break away; thus, the stent is no longer restrictive (Fig. 21.3).
< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


