Prosthetic Valves and Rings
Prosthetic valves may be made from metal and other material or may be biologic grafts (i.e., heterografts, homografts, or autografts). Mechanical grafts last longer than bioprostheses but require long-term anticoagulation. The potential advantage of the bioprostheses is that anticoagulation is required only early after placement unless indicated for other reasons, such as the presence of atrial fibrillation. Porcine heterografts are the most commonly used ones; they cannot be implanted in children, however, because of the relatively rapid calcification that occurs. Homografts (i.e., human valves) and autografts (i.e., grafts from the same individual—as in the placement of the pulmonary valve in the aortic position) may be less prone to calcification. The Ross procedure is a recently developed surgical approach in which the patient’s pulmonary valve is placed in the aortic position and a homograft is placed in the pulmonary position. The lower pressure gradient across the homograft in the pulmonary position may make it less prone to calcification. An important role of transesophageal echocardiography is to measure the size of the annulus to be certain that appropriately sized homografts are available and, in the case of the Ross procedure, to be certain that the pulmonary valve is of the right size for placement in the aortic position.
The most commonly used mechanical valve is the St. Jude valve. Newer valves such as the Carbomedics (Sulzer Carbomedics Inc., Austin, TX) and Medtronic-Hall (Meditronics, Inc., Minneapolis, MN) valves are preferred by some surgeons, and their use is increasing. The echocardiographer must also be familiar with other valves, such as the Bjork-Shiley and Starr-Edwards valves, because large numbers of these implants are still functioning.
Problems that can occur with all valves include paravalvular leaks, infection, and thrombus. Bioprosthetic valves may also calcify and degenerate.
Because all mechanical and bioprosthetic valves are inherently a little stenotic, a region of flow acceleration can often be seen proximal to the valve during the flow across the valve. Because of the presence of localized areas of high-velocity flow, the Doppler study may overestimate the gradient across the prosthetic valve. The assessment of the prosthetic valve stenosis must therefore be approached with great caution, and published tables giving normal ranges for various prosthetic valves are not very helpful. The problem is further complicated by prosthesis–patient mismatch seen in some patients. Therefore, high-pressure gradients noted across prosthetic valves, especially metallic ones, do not necessarily imply obstruction. Because of this, measurement of prosthetic orifice areas using the Doppler continuity equation or pressure half-time method may not be accurate. A baseline study performed at the time of surgery can be helpful so that changes in pressure gradients can be followed up over time. It is important to investigate the motion of the occluder or leaflets when assessing stenosis. Immediately after the termination of cardiopulmonary bypass, the flow may be inadequate to open one of the leaflets of the mechanical prosthetic valve. This is a normal finding that resolves over time as cardiac output increases. For valves in the mitral position, a flat EF slope in association with a high velocity on conventional Doppler study suggests obstruction.
Valve prostheses may normally have a small amount of regurgitation. In the case of the St. Jude and CarboMedics valves, up to three small regurgitant jets are seen. These correspond to the two leaflets and to a central jet. Compared with pathologic regurgitant jets, these normal jets tend to be more laminar and narrow. In mitral prostheses the jets may, however, extend well into the left atrium. In assessing the severity of the prosthetic mitral regurgitation, it is important to investigate the pulmonary veins near their entry into the left atrium with the conventional Doppler to search for systolic backflow, which is a reliable marker for severe regurgitation. The size of the proximal flow acceleration should also be assessed. Finally, the area of the jet is important (<4 cm2, mild regurgitation; 4 to 8 cm2, moderate regurgitation; >8 cm2, severe regurgitation), although jet area may be misleading if an eccentric jet is present. Multiple planes
should be interrogated to find the plane in which the regurgitant jet has the largest area. The Nyquist limit should be kept between 40 and 50 cm/sec. Changes in the Nyquist limit, and consequently the wall filter, will affect the jet area. The spontaneous contrast in the left atrium suggests that any mitral regurgitation is not severe. In the case of aortic prostheses, the aortic regurgitant jet may be seen best by the transthoracic approach because there is acoustic shadowing of the jet on the transesophageal examination, caused by the metallic components and posterior calcification. For prostheses in the aortic position, the severity of the regurgitation is assessed by determining the ratio of jet width at its origin to left ventricular outflow tract diameter, also measured at the origin of the jet (<38%, mild; 39% to 75%, moderate; >75%, severe).
should be interrogated to find the plane in which the regurgitant jet has the largest area. The Nyquist limit should be kept between 40 and 50 cm/sec. Changes in the Nyquist limit, and consequently the wall filter, will affect the jet area. The spontaneous contrast in the left atrium suggests that any mitral regurgitation is not severe. In the case of aortic prostheses, the aortic regurgitant jet may be seen best by the transthoracic approach because there is acoustic shadowing of the jet on the transesophageal examination, caused by the metallic components and posterior calcification. For prostheses in the aortic position, the severity of the regurgitation is assessed by determining the ratio of jet width at its origin to left ventricular outflow tract diameter, also measured at the origin of the jet (<38%, mild; 39% to 75%, moderate; >75%, severe).
Paravalvular leaks may be important causes of regurgitation. These leaks may be caused by valve suture dehiscence and can be seen to originate beyond the extent of the prosthetic elements. The location of proximal flow acceleration outside the confines of the prosthesis may also help determine if the leak is paravalvular.
Thrombi can lead to emboli or to obstruction or may interfere with the function of a valve and cause significant regurgitation. Thrombi may be present in the left atrium or left atrial appendage and may well be seen on the transesophageal study. Because the left atrial appendage may be partially or completely removed at the time of surgery, inability to image it should not be taken as evidence that there is a clot obscuring the appendage. Left ventricular function is better preserved if the papillary muscles are not completely removed; remnants of the papillary muscle and chordae left in place by the surgeon may be mistaken for a mobile clot. For this reason, a baseline transesophageal study is of great use for comparison.
Transesophageal and transthoracic examinations are complementary in patients with a mitral valve replacement. Transesophageal study is far more effective than is transthoracic examination in assessing the left atrium for the presence and severity of mitral regurgitation in patients with valves in the mitral position. On transthoracic study, acoustic shadowing of the left atrium by the valve is observed. Conversely, substantial acoustic shadowing and reverberation that degrade the transesophageal image of the left ventricle are present on transesophageal study but not on transthoracic examination.
Certain structures are well examined by transesophageal echocardiography. The short-axis view of a prosthetic valve permits a complete view of the valve suture line. Stents are well seen, and, in the case of mitral prostheses, may physically narrow the left ventricular outflow tract or may impinge on the left ventricular free wall or ventricular septum, producing arrhythmias or conduction system abnormalities. Bioprosthetic mitral cusp rupture resulting from degeneration or infection may be manifested as linear echoes protruding into the left atrium, with or without fluttering. Left atrial perforation or dissection may be seen. Abscesses may be visualized. They may be large and filled with pus. The presence of flow signals in the abscess cavity demonstrates that there is communication with an adjoining vessel or cavity. Abscesses may form fistulas to other structures. Following aortic valve replacement, systolic anterior motion of the mitral valve may be unmasked, and significant left ventricular outflow tract obstruction may develop in the presence of coexisting hypertrophic cardiomyopathy. Rarely, a left ventricular outflow tract gradient may be caused by an abscess narrowing the outflow tract. Pannus may cause obstruction and may be difficult to distinguish from clot. If the obstructing echo density is mobile and less dense thrombus is more likely. Bioprosthetic valves may suffer cusp degeneration or calcification, which may produce obstruction. Linear echoes protruding into the left ventricular outflow tract are characteristic of prolapse caused by bioprosthetic aortic valve degeneration. Similar echoes may also be caused by infection.
Transesophageal echocardiography is also useful in the assessment of mitral annuloplasty rings, which are placed to reduce the severity of mitral regurgitation. Residual mitral regurgitation, as well as ring thrombus, obstruction, and dehiscence, are well demonstrated. Systolic anterior motion of the anterior mitral leaflet with left ventricular outflow tract obstruction may also occur after ring placement and can be diagnosed by echocardiography. In patients undergoing aortic valvuloplasty, the site of aortic valve repair and the severity of residual aortic regurgitation are also well assessed by transesophageal echocardiography.
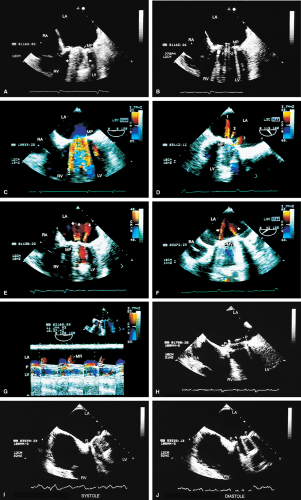 FIGURE 5.1. St. Jude mitral prosthesis: normal. The mitral prosthesis (MP) is seen in the closed (A) and open (B) positions. A. Prosthetic reverberations or artifacts (arrows) that clutter the left ventricle (LV). B. The two leaflets (1 and 2) of the prosthesis in the open position together with the reverberations. C. Aliased diastolic inflow into the LV is seen with a small region of flow acceleration. D–G. Two to three small jets of mitral regurgitation (MR; arrows) are shown. These are normal findings. Usually, these jets are narrow and do not show significant turbulence but may extend deep into the left atrium (LA). G. illustrates the norm (not pansystolic). H. Small linear echoes are normally seen on both the atrial and ventricular aspects of the prosthesis and represent suture material. I, J. Immediately postsurgery, although the patient is still on partial bypass, one leaflet of the prosthesis (P) may intermittently fail to open. This should not be mistaken for dysfunction. When cardiac output improves, normal opening of both leaflets occurs consistently. RV, right ventricle; RA, right atrium. |
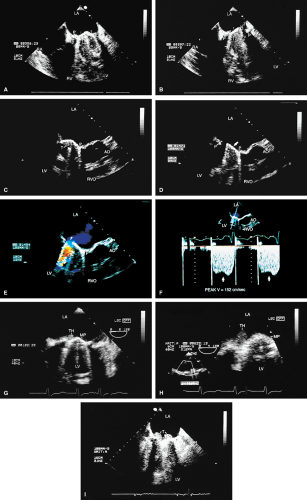 FIGURE 5.2. St. Jude mitral prosthesis: thrombus. A–F. Localized echo densities consistent with thrombus (T) are noted on the St. Jude prosthesis (P) in two different patients (A,B and C–F). In both patients, thrombus prevented the opening of one of the leaflets of the prosthesis. F. Continuous wave Doppler shows a flat velocity profile in early diastole (arrows) and a high peak velocity of 152 cm/sec consistent with obstruction. G and H (one patient) and I (another patient) show two other patients with thrombosed (TH, T) St. Jude mitral prostheses. The echo densities representing thrombus are seen on the atrial side of the prosthesis. Thrombi are less dense than the metallic components of the prosthesis and are different from prosthetic reverberations, which are anteriorly directed, more prominent, and have larger linear echoes. In addition, reverberations are not seen on the atrial aspect of the prosthesis. AO, aorta; LA, left atrium; LV, left ventricle; MP, mitral prosthesis; RA, right atrium; RV, right ventricle; RVO, right ventricular outflow tract. |
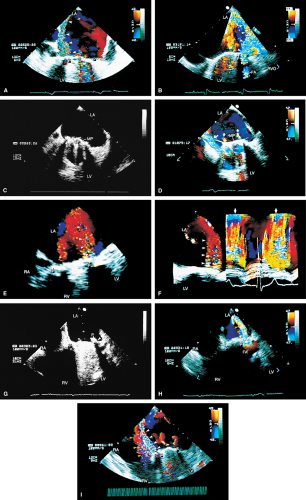 FIGURE 5.3. St. Jude mitral prosthesis: paravalvular regurgitation. A. A large eccentric jet (arrowheads) coursing medially along the atrial septum is seen originating beyond the edges of the prosthetic elements (P). B. The paraprosthetic leak (arrowheads) is located laterally. There is also a large zone of flow acceleration (FA), which is clearly located outside the confines of the prosthetic valve (P). C. The dehisced area (arrow) is clearly seen, and a wide jet of paravalvular regurgitation (oblique arrow) can be seen coursing through it (D). The vertical arrows point to two small jets of normal valvular regurgitation through the St. Jude prosthesis. E,F. Another patient with dehiscence of sutures and pansystolic paravalvular regurgitation. G,H. Another patient with suture dehiscence (arrow in G) and severe eccentric MR (arrowheads), with a large FA on the ventricular aspect of the St. Jude prosthesis. I. There is eccentric periprosthetic MR (white arrows) as well as eccentric TR (yellow arrows) moving along the atrial septum. Two small normal jets of MR also are seen originating from the St. Jude prosthesis. LA, left atrium; LV, left ventricle; MP, mitral prosthesis; RA, right atrium; RV, right ventricle; RVO, right ventricular outflow tract. |
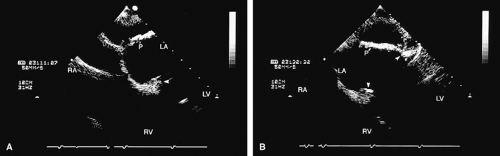 FIGURE 5.4. A,B. St. Jude mitral prosthesis: ectopic position. In this patient, the St. Jude prosthesis (P) is attached to the wall of the left atrium (LA) (upper arrowhead in B) rather than to the valve ring (lower arrowheads). LV, left ventricle; RA, right atrium; RV, right ventricle. |
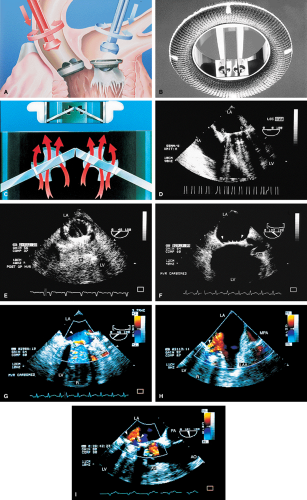 FIGURE 5.5. CarboMedics mitral prosthesis: normal. A–C. Schematics of the CarboMedics mitral prosthesis. In A, the CarboMedics aortic prosthesis is also shown. C. The mechanism of normally occurring MR through the hinge points (courtesy of Sulzer CarboMedics Inc., Austin, TX). D. The prosthesis is seen in the four-chamber view, demonstrating multiple reverberations (1, 2, 3, 4) partially obscuring the left ventricle (LV) and right ventricle (RV) cavities. E. Both leaflets of the prosthesis and the suture ring (arrow) are viewed in the short axis. F. Individual sutures (arrowheads) are seen on the atrial aspect of the prosthetic valve. G. Diastolic flow acceleration (arrowhead) on the atrial aspect of the prosthesis. The LV inflow jet is large. H,I. Two small jets of normal prosthetic valvular regurgitation (arrowheads). R, prosthetic reverberations. AO, aorta; AV, aortic valve; LA, left atrium; LAA, left atrial appendage; MPA, main pulmonary artery; PA, pulmonary artery; RA, right atrium; VS, ventricular septum. |
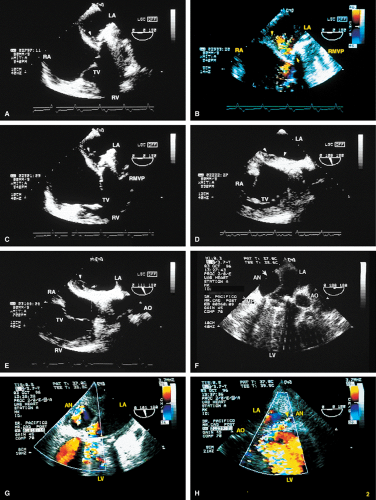 FIGURE 5.6. A–E. CarboMedics mitral prosthesis: dehiscence of left atrium (LA) wall. A. A small linear echo (vertical arrow) at the site of the paravalvular defect (horizontal arrow) consistent with suture material. B. Color Doppler examination shows a large paravalvular regurgitant jet originating at the site of the paravalvular defect (arrow) shown in A. C. An abnormal 1-cm linear echo (arrow) protrudes into the LA at the midinteratrial septal level. D,E. Multiplane views at 105° and 111° demonstrate a cavitary defect (arrows) involving the LA wall at the midinteratrial septal level, indicative of dehiscence, which explains the presence of the linear echo in the LA seen in C. F–H. CarboMedics mitral prosthesis (MP): LA pseudoaneurysm. F. A large pseudoaneurysm (AN; arrow) that developed following prosthetic replacement (MP, arrowhead) of the mitral valve. G,H. Color Doppler examination shows flow signals (arrowhead in H) moving from the left ventricle (LV) into the aneurysm cavity. AO, aorta; RA, right atrium; RMVP, reverberations from mitral valve prosthesis. (A–E reproduced with permission from Howard J, Agrawal G, Nanda NC. Transesophageal echocardiographic diagnosis of left atrial wall dehiscence. Echocardiography 1997;14:299–302. ) |
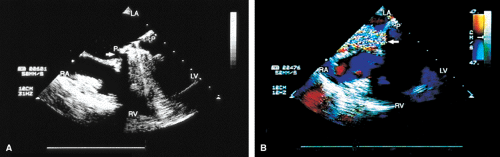 FIGURE 5.8. Bjork-Shiley mitral prosthesis: suture dehiscence. The arrow in A shows a large area of dehiscence with severe paraprosthetic (P) MR (arrow in B). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. |
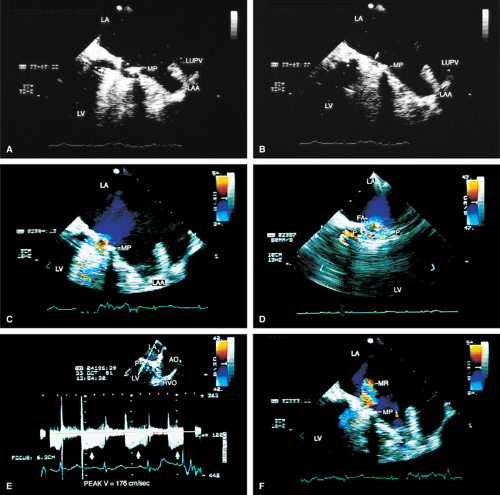 FIGURE 5.9. Cooley-Cutter mitral prosthesis: stenosis. A. Prosthetic reverberations (arrow). B. A questionable thrombus (arrow). C,D. Prominent flow acceleration (FA) is present on the atrial aspect of the prosthesis (MP, P). E. A high velocity of 176 cm/sec was measured across the prosthesis by continuous wave Doppler (arrows). F. Associated mild mitral regurgitation (MR). AO, aorta; LA, left atrium; LAA, left atrial appendage; LUPV, left upper pulmonary vein; LV, left ventricle; MP, mitral prosthesis; MR, mitral regurgitation; RVO, right ventricular outflow tract. |
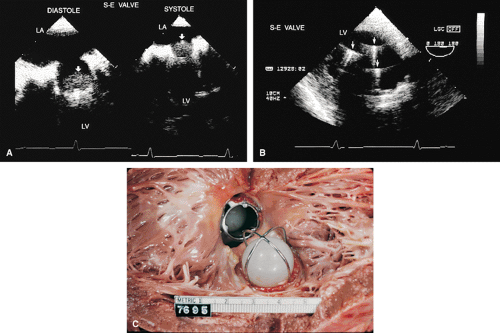 FIGURE 5.10. Starr-Edwards prosthesis: normal. A. The rounded poppet (arrows) is seen in the open position in diastole and in the closed position in systole. B. Transgastric view shows the three prosthetic struts (arrows) together with the resulting reverberations imaged in short axis. C. Gross specimen shows Starr-Edwards prostheses in the aortic and mitral positions. LA, left atrium; LV, left ventricle. |
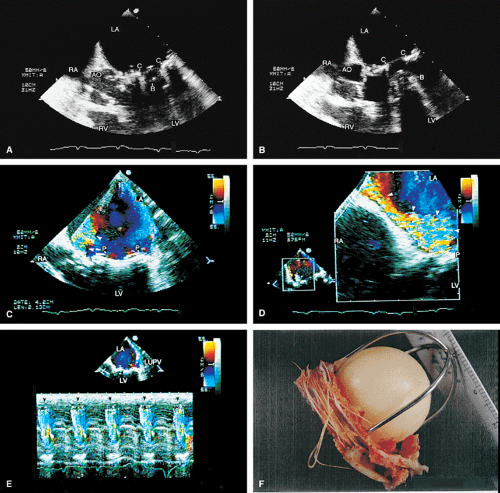 FIGURE 5.11. Starr-Edwards mitral prosthesis: dehiscence. The poppet, or ball (B), is seen in the closed (A) and open (B) positions. Note the reverberations from the ball partially obscuring the left ventricle (LV) in B. C,D. Eccentric, severe paravalvular mitral regurgitation (arrowheads) originating beyond the prosthetic (P) elements is shown. E. Color M-mode examination demonstrates systolic backflow (arrowheads) in the left upper pulmonary vein (LUPV), confirming the presence of severe MR. C, C, mitral ring. F. Gross specimen shows suture dehiscence and clot involving a Starr-Edwards prosthesis. AO, aorta; LA, left atrium; RA, right atrium; RV, right ventricle. |
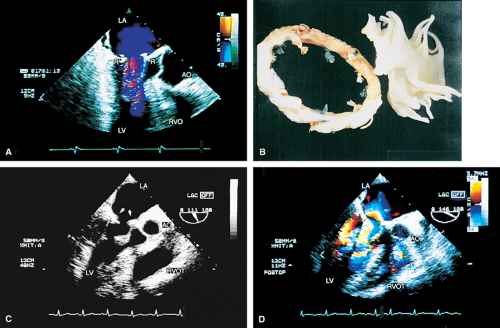 FIGURE 5.12. Mitral annuloplasty rings. A. R points to the Carpentier ring in the mitral position. There is no obstruction to mitral flow. B. Gross specimen of Carpentier ring. C,D. Duran ring in the mitral position (arrows in C). D. Color Doppler examination shows prominent flow acceleration and aliased flow resulting from narrowing of the mitral orifice by the ring. AO, aorta; LA, left atrium; LV, left ventricle; RVO, RVOT, right ventricular outflow tract. |
 FIGURE 5.13. Mitral annuloplasty ring. A. R demonstrates an annuloplasty ring in the mitral position. S, sutures. B. Color Doppler examination shows aliased inflow signals and prominent diastolic flow acceleration (arrow) produced by narrowing of the mitral orifice by the ring. C. Pulsed-Doppler examination of the left upper pulmonary vein (PV) shows a smaller S wave than D wave, consistent with moderate mitral regurgitation (MR) preoperatively. After ring placement, the S wave is equal to the D wave, suggesting a reduction in mitral regurgitation (in D). E. Another patient in whom the annulus size was reduced to 2.64 cm after placement of an annuloplasty ring for severe MR. LA, left atrium; LV, left ventricle, RV, right ventricle. |
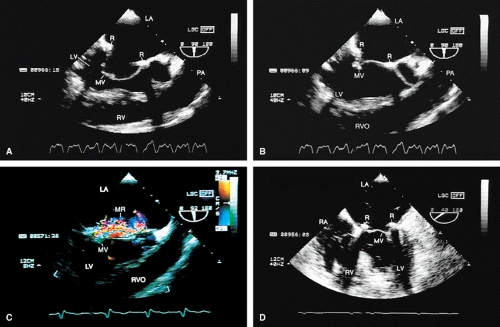 FIGURE 5.14. Mitral annuloplasty ring. The ring (R) is seen in diastole in A and in systole in B. C. Color Doppler examination shows moderate residual mitral regurgitation (MR) in this patient, who had severe MR before ring placement. D. A systolic frame shows ring (R) echoes in another patient following mitral annuloplasty. LA, left atrium; LV, left ventricle; MV, mitral valve; PA, pulmonary artery; RV, right ventricle; RVO, right ventricular outflow tract. |
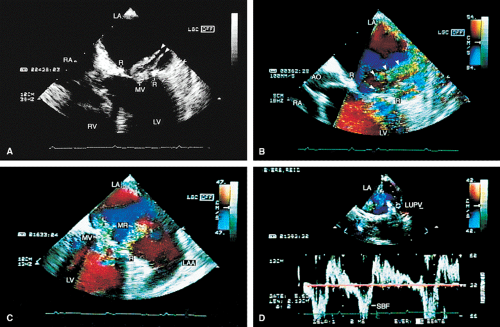 FIGURE 5.15. Mitral annuloplasty ring: ruptured chordae. A. Ruptured chordae (arrowheads) prolapsing into the left atrium (LA) in systole. R, mitral annuloplasty ring. B,C. Color Doppler examination demonstrates severe eccentric mitral regurgitation (MR) (arrowheads) through the ring with prominent systolic backflow (SBF) in the LUPV (D). AO, aorta; LAA, left atrial appendage; LUPV, left upper pulmonary vein; LV, left ventricle; MV, mitral valve; RA, right atrium; RV, right ventricle. |
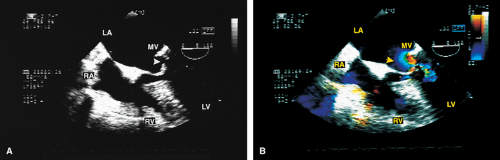 FIGURE 5.16. Mitral annuloplasty ring: obstruction. A,B. Prominent diastolic flow acceleration (arrow) and a narrow inflow jet resulted from obstruction produced by a Duran ring in this patient. LA, left atrium; LV, left ventricle; MV, mitral valve; RA, right atrium; RV, right ventricle. |
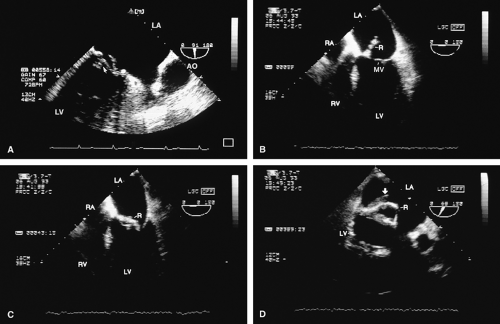 FIGURE 5.17. Mitral annuloplasty ring: thrombus/dehiscence. A. A thrombus (arrow) involving the ventricular aspect of a Duran ring. There is severe mitral valve (MV) prolapse. B–D.
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|